Study design
This was a multicenter, phase 1b/2 clinical trial (NCT04019327) comprising a maximum tolerated dose (MTD) determination lead-in phase (phase 1b) followed by an open-label, single arm, interventional signal-finding study of intermittent talazoparib plus temozolomide (phase 2).
Dose escalation was carried out using the modified toxicity probability interval-2 (mTPI-2) method [11]. The phase 1 starting dose was 1 mg once daily (QD) for talazoparib (Days [D] 1–6 of 28-day cycles) along with 37.5 mg/m2 QD for temozolomide (D2-8 of 28-day cycles). Subsequent doses were assessed (see Results and Table 1), with the maximum assessed dose being talazoparib 1 mg QD (D1-6) and temozolomide 75 mg/m2 QD (D2-8). Patients were treated in cohorts of 3. The mTPI-2 matrix was applied to all patients on the current dose level to decide whether to escalate, de-escalate or stay at the current level for the next cohort of patients. Dose reductions for toxicity of both talazoparib and temozolomide were defined in the protocol. Growth factor support with pegfilgrastim was allowed.
Table 1 Patient demographic and clinical characteristics by dose level characteristicThis study was approved by an institutional review board at each participating site and was conducted in accordance with Good Clinical Practice guidelines, defined by the International Conference on Harmonisation. All patients provided written informed consent.
Choice of starting dose
The pulse dosing of talazoparib D1-6 with temozolomide D2-8 was based in part on the long half-life of talazoparib. One day is required to obtain trough concentration levels > 2 ng/mL of talazoparib based on exposure–response data before starting temozolomide. These trough concentration levels would be expected to be maintained for another 4 days after stopping talazoparib, or effectively until D10 of each cycle. The duration of the cycle was based upon expected time for marrow recovery.
Patient eligibility
Eligible patients were males ≥ 18 years old with a histologically or cytologically confirmed adenocarcinoma of the prostate whose tumors did not harbor alterations in homologous recombinant repair (HRR) HRR was determined using a Clinical Laboratory Improvement Amendments (CLIA)-certified next generation sequencing assay from archival or fresh tumor tissue in addition to germline testing. Testing was done using MSK-IMPACT (Memorial Sloan Kettering Integrated Mutation Profiling of Actionable Cancer Targets, New York, NY) or Tempus (Tempus AI, Inc., Chicago, IL) and results were centrally reviewed. Patients with pathologic somatic or germline mutations in BRCA1, BRCA2, ATM, FANCA, CHEK2, PALB2, MRE11A, NBN, RAD51C, ATR, or cMLH1 were excluded.
Eligible patients with mCRPC must have had progression on treatment with abiraterone acetate with prednisone and/or enzalutamide. Progression was based on either PSA progression defined as at least 2 rises in PSA with a minimum of a 1-week interval, soft tissue progression per Response Evaluation Criteria in Solid Tumors (RECIST) v1.1, or progression of bone disease by bone scan per Prostate Cancer Clinical Trials Working Group 3 (PCWG3) criteria [12]. Metastatic disease was documented by bone lesions on whole-body radionuclide bone scan, and soft tissue disease by computed tomography or magnetic resonance imaging (CT/MRI). RECIST-measurable disease was not required.
Patients had an Eastern Cooperative Oncology Group (ECOG) performance score of 0 or 1, and serum testosterone ≤ 50 ng/dL. Patients had adequate bone marrow, renal and hepatic function as follows: absolute neutrophil count (ANC) ≥ 1,500/µL, platelets ≥ 100,000/µL, hemoglobin ≥ 9.0 g/dL, serum creatinine clearance ≥ 60 mL/min estimated using the Cockcroft-Gault equation, and aspartate aminotransferase (AST) and alanine aminotransferase (ALT) ≤ 2.5 × the upper limit of normal (ULN). Patients with prior treatment with a taxane-based chemotherapy for mCRPC, prior treatment with a PARP inhibitor, platinum, cyclophosphamide, mitoxantrone, or temozolomide were excluded. Prior docetaxel chemotherapy in hormone-sensitive disease was allowed.
Objectives and assessments
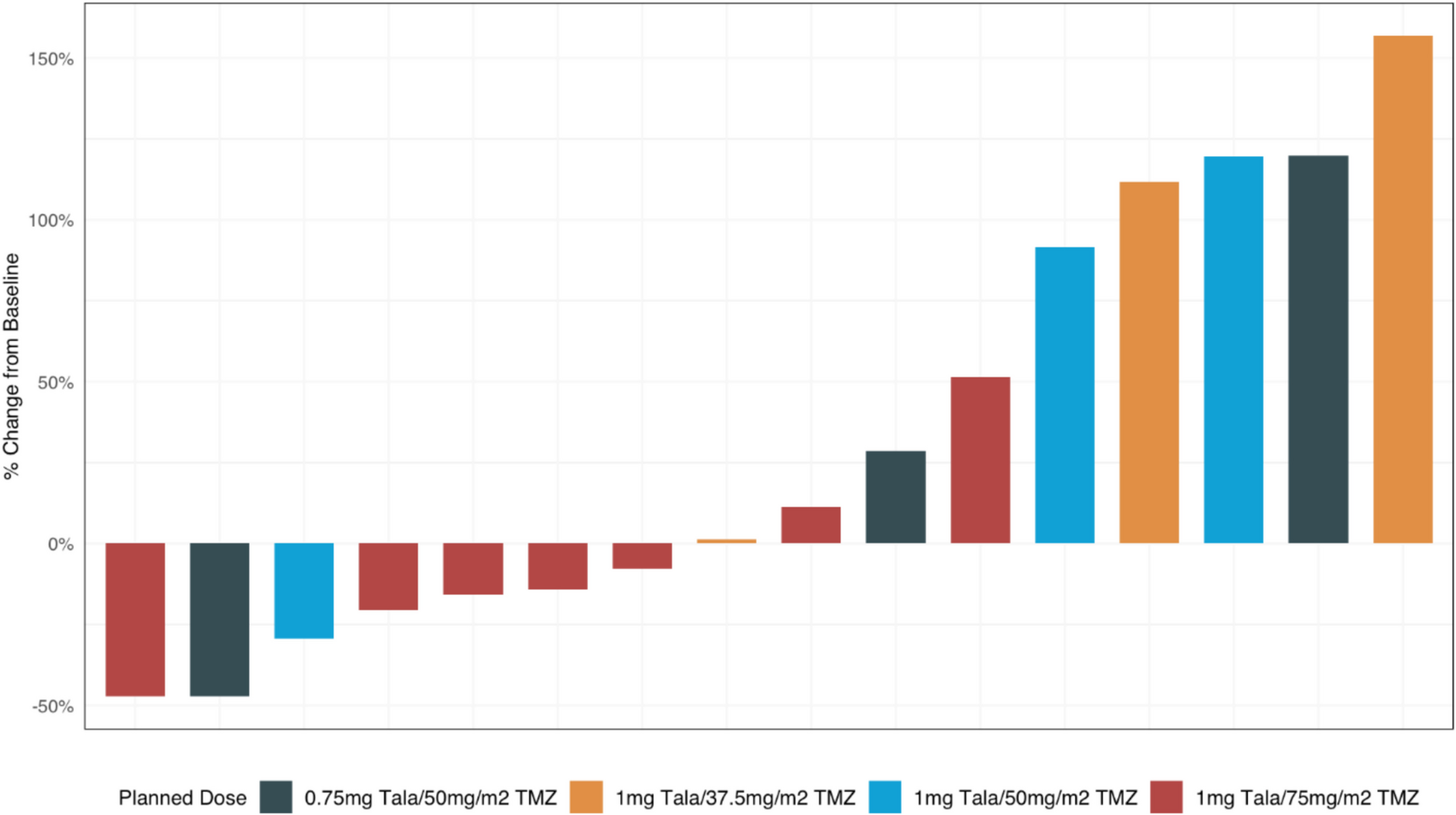
The primary objective of the phase 1b trial was to determine the safety, MTD, and RP2D of intermittent talazoparib plus temozolomide in patients with mCRPC whose tumors did not harbor mutations in HRR. The primary objective of phase 2 was to determine efficacy using a composite endpoint. Response was defined as any one or more of the following: confirmed complete response (CR) or partial response (PR) according to RECIST v1.1, reduction in prostate-specific antigen (PSA) level of ≥ 50% from baseline/pre-treatment, and/or circulating tumor cells (CTC) conversion, defined as a reduction in the number of CTCs from ≥ 1 per 7.5 mL of blood at baseline to 0 per 7.5 mL during treatment using the CellSearch assay (Menarini Silicon Biosystems, Inc., Huntingdon Valley, PA). Correlative objectives for this phase 1b/2 study also included the evaluation of patient-reported toxicity using select items on the National Cancer Institute’s (NCI) Patient-Reported Outcomes version of the Common Terminology Criteria for Adverse Events (PRO-CTCAE), and biomarker analyses including evaluation of Schalfen 11 (SLFN11) expression on tumor tissue. Immunohistochemical (IHC) staining for SLFN11 was performed on formalin-fixed, paraffin-embedded (FFPE) tissue sections of archival or fresh prostate biopsy samples, as well as metastatic biopsy tissues as previously described but with use of the automated Leica BOND platform according to the manufacturer’s instruction [13]. All slides were examined under light microscopy by a qualified pathologist for staining intensity and percentage of stained cells to determine H-score.
Safety assessments included evaluation of NCI’s Common Terminology Criteria for Adverse Events (CTCAE) v5.0. PRO-CTCAE captured select patient toxicities on cycle (C) 1, day (D) 1, C1D15, C2, C3, C5, C7, and end of treatment (EOT). The PRO-CTCAE items assessed were decreased appetite, nausea, shortness of breath, numbness or tingling in hands or feet, dizziness, pain, headache, and fatigue.
Circulating tumor DNA (ctDNA) was collected at screening, C2, C3, C5, and EOT. CTCs and PSA were measured at screening and the start of each cycle.
Laboratory assessments for safety (complete blood count with differential, comprehensive metabolic panel) were performed weekly in the first cycle, biweekly in the second cycle, then monthly at the start of each cycle. Imaging with CT or MRI and bone scan were performed every 8 weeks.
The dose-limiting toxicity (DLT) period was defined as the first cycle (through 28D) and included hematologic toxicity (e.g., neutropenic fever of any duration, grade 4 neutropenia lasting more than 7D despite support, grade 4 thrombocytopenia, grade 3 thrombocytopenia with bleeding, or grade 4 anemia lasting more than 72 h despite transfusion support) and non-hematologic toxicity parameters (grade 3 treatment-related adverse events (AEs) considered clinically significant).
Statistical analyses
The study was anticipated to enroll up to 55 patients with up to 30 patients in phase 1b and a total of 35 treated at the RP2D (in both phase 1b and phase 2). The study was designed to enroll 19 patients at the MTD in the first stage of the phase 2 portion of the trial. If 4 or fewer patients met the primary response endpoint, the trial would be terminated for futility. If not, then an additional 16 patients would be enrolled for a total of 35 patients treated at the RP2D.
This trial used a two-stage design with 1-sided alpha of 0.05 and 80% power. If the response rate was 35% or higher, the combination would be considered promising, and not promising if the response rate was 15% or lower.





Comments (0)