This retrospective, real-world study demonstrated that semi-dose VEN (200 mg/d) combined with AZA achieved exceptional outcomes in elderly and frail AML patients in China. The findings indicated that this 200 mg/day VEN-AZA regimen possessed potent antileukemic efficacy and a favorable safety profile, with a median OS exceeding 24.6 months.
AML is a disease with significantly increased incidence in the elderly population, and the median age at diagnosis of approximately 69 years [13]. Older patients often have adverse genetics/comorbidities and poor prognosis, mainly due to intolerance to intensified therapy and/or treatment resistance [14, 15]. VEN-AZA offers a new therapeutic approach for elderly/unfit AML patients [4]. This synergy effect arises from VEN targeting BCL-2, which is crucial for AML blasts survival [16], while AZA reduces MCL-1 levels, a key resistance factor to VEN [17].
Historically, CR/CRi rates for unfit AML patients receiving VEN-AZA in clinical trials range from 66.4% to 71%, with median OS of 14.7–16.4 months and median EFS of 9.8 months [3, 4, 17]. These data predominantly originate from randomized controlled trials (RCTs), whereas real-world cohorts exhibit distinct disease characteristics and include trial-ineligible patients. International real-world studies report lower CR/CRi rates (34.2–48.8%), median OS (6.3–12.7 months), and median EFS (5.8–9.5 months) [18, 19]. Chinese real-world data align with these findings, demonstrating CR/CRi rates of 44.9–68.8%, median OS of 9.1–11.93 months, and median EFS of 5.2–11.5 months [5, 20]. This OS reduction in real-world settings is attributable not only to poorer baseline characteristics and higher-risk disease features but also to reduced treatment tolerance and therapy discontinuation due to AEs. Critically, achieving CR/CRi and completing ≥ 6 treatment cycles are established predictors of improved OS [21, 22].
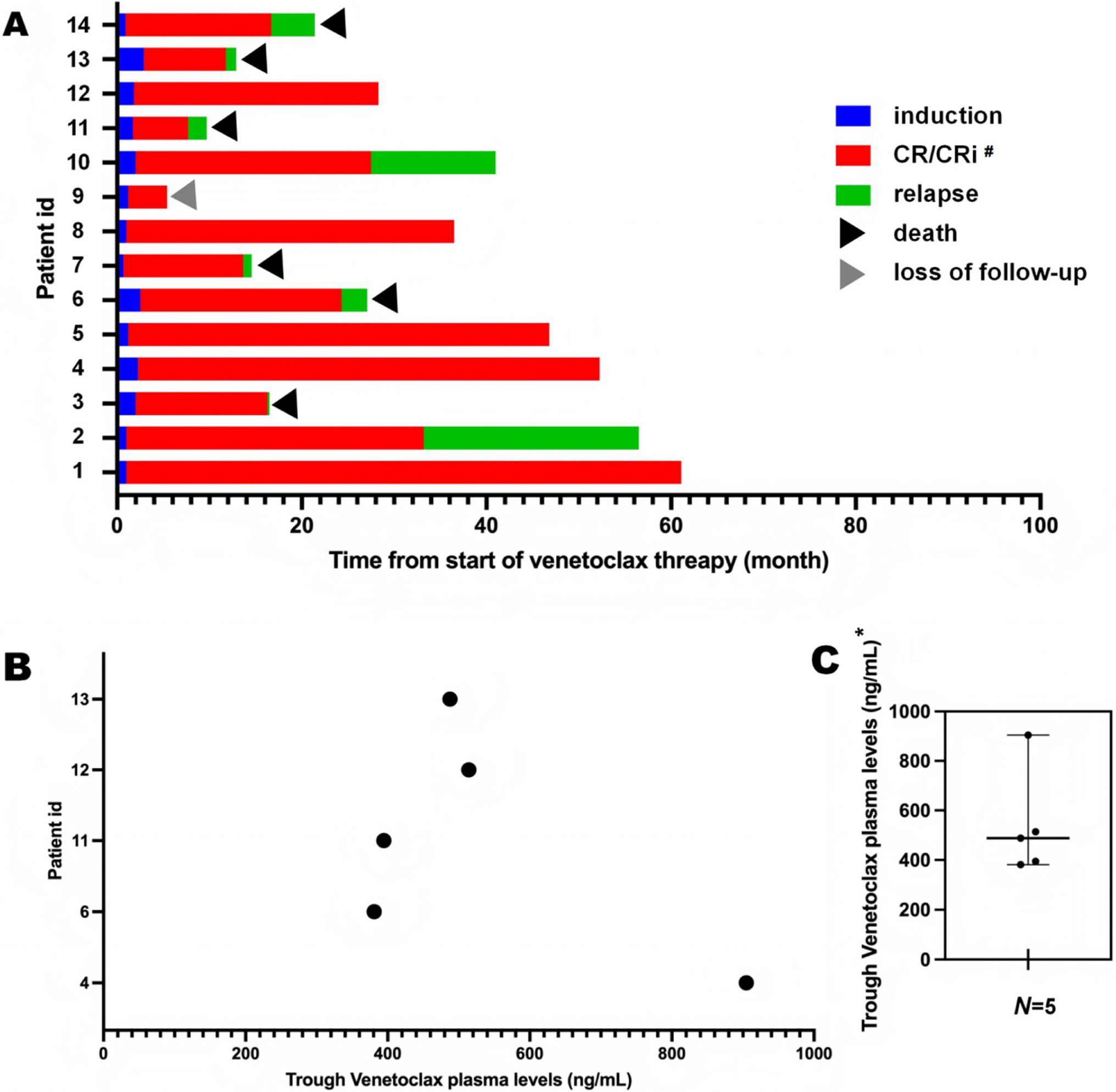
Our cohort exhibited particularly adverse features. Patients enrolled characterized by advanced age (median 71.5 years), poor performance status (64.3% ECOG ≥ 3), and adverse disease biology (57.1% ELN adverse-risk, 57.1% bone marrow blasts > 50.0%). All 14 patients (including one relapsed AML case) completed ≥ 4 cycles of reduced-dose VEN (200 mg/day) plus AZA. Remarkably, a 100% CR/CRi rate was achieved, exceeding historical outcomes with full-dose (400 mg/day) regimens. Rapid response was observed, with median time to MRD negativity only 1.45 months, enabling early disease control. Survival outcomes were robust: median EFS reached 23.6 months (95% CI 15.8–32.2), while median OS was not reached (> 24.6 months). The 2-year OS and EFS rates were 61.5% and 53.8%, respectively. Notably, 50.0% of adverse-risk patients survived beyond 21.8 months, challenging conventional expectations for this subgroup where median OS typically falls below 12 months with conventional low-intensity therapies [23].
The efficacy of reduced-dose VEN is pharmacokinetically supported. Phase III data indicate 67% higher mean relative bioavailability in Asian versus non-Asian patients [24], suggesting enhanced drug absorption in Chinese patients. Our therapeutic drug monitoring (TDM) confirmed median trough concentrations of 487.7 ng/mL (IQR 394.7–514.1), approximating the therapeutic threshold for BCL-2 inhibition (~ 500 ng/mL). This observation validates ethnically driven metabolic variations, proving therapeutic efficacy at reduced systemic exposures. Notably, all measured concentrations (range, 380.9–904.7 ng/mL) met or exceeded the target range despite interindividual variability. Notably, no significant correlation emerged between VEN concentration and survival outcomes (p > 0.05). This pattern likely indicates universally adequate target exposure rather than pharmacological inefficacy. However, the analysis was underpowered due to the small TDM cohort (n = 5), limiting comprehensive pharmacokinetic-pharmacodynamic assessment.
Compared to standard-dose VEN-AZA regimens, our reduced-intensity (semi-dose) protocol demonstrated a significantly improved hematologic safety profile in real-world Chinese patients. While pivotal clinical trials of full-dose VEN-AZA reported grade 3/4 febrile neutropenia (20–43%), anemia (25–30%), and thrombocytopenia (24–45%) [3, 4, 17], and Chinese real-world studies of full-dose regimens showed even higher incidences (febrile neutropenia: 42.9–78.9%; anemia: 70–100%; thrombocytopenia: 65.6–89.5%) [5, 20], our semi-dose regimen achieved markedly lower rates of severe hematologic toxicity: febrile neutropenia (35.7%), anemia (50.0%), and thrombocytopenia (21.4%). Crucially, our thrombocytopenia incidence fell below the lower bound of both clinical trial data (21.4% vs 24–45%) and real-world benchmarks (21.4% vs 65.6–89.5%), representing a particularly striking reduction. Similarly, our febrile neutropenia rate was substantially lower than the minimum reported in Chinese real-world studies (35.7% vs 42.9–78.9%). Although grade ≥ 3 neutropenia remained relatively high (64.3%), it was comparable to the lower end of full-dose real-world ranges (31–91.2%) [5, 20]. The all-grade pneumonia rate (28.6%) also aligned with grade 3/4 rates in full-dose trials (13–32%) [3, 4, 17].
Our analysis showed median recovery times of ~ 33 days for both ANC and PLT, indicating that reduced-dose VEN-AZA enables hematopoietic recovery within about one month, comparable to or faster than the 4–6 weeks typically reported with full-dose regimens [3]. Critically, all responders maintained blood counts above safety thresholds (ANC > 0.5 × 109/L, PLT > 50 × 109/L) throughout 48-month follow-up, suggesting a potential safety advantage. Nonetheless, these results should be interpreted cautiously and require validation in larger cohorts.
Besides, molecular analyses revealed differential treatment responses. Patients with IDH1/2 mutations (n = 3) exhibited exceptional outcomes with no OS/EFS events and all surviving > 26.5 months, aligning with mechanistic studies demonstrating synergistic BCL-2 inhibition and epigenetic modulation in this subtype. Conversely, patients with DNMT3A mutations (n = 5) experienced markedly inferior outcomes (80% OS/EFS events), frequently associated with elevated baseline marrow blast burden (39–80%). This observation resonates with reports linking DNMT3A mutations to reduced sensitivity to hypomethylating agents [25], suggesting an unmet need for augmented therapeutic strategies in this subgroup.
This study has several limitations that should be acknowledged. First, the retrospective, single-center design and very small sample size (n = 14) inevitably restrict statistical power and may introduce selection bias, thereby limiting the generalizability of our findings. The heterogeneous follow-up duration further constrains the robustness of subgroup analyses. Second, only one patient in our cohort had relapsed/refractory AML, which weakens the applicability of our conclusions to this subgroup. Third, there was no concurrent control group treated with the full-dose venetoclax plus azacitidine regimen, which reduces the persuasiveness of directly challenging the necessity of the standard dose. To partially address this, we compared our outcomes with historical data from pivotal trials and large-scale real-world studies, although such cross-study comparisons must be interpreted with caution due to differences in patient populations and study design.
Another limitation relates to pharmacokinetic assessment and follow-up indicators. The analysis of VEN trough concentrations was based on only five patients, precluding any reliable conclusions regarding the relationship between drug exposure and survival outcomes. In addition, TDM of VEN is not routinely available in most Chinese hospitals, reflecting real-world barriers to comprehensive pharmacokinetic-pharmacodynamic analyses. Furthermore, long-term quality-of-life (QoL) outcomes were not systematically assessed during follow-up, limiting our ability to evaluate the broader impact of reduced-dose VEN-AZA on functional status and patient well-being.
Finally, the subgroup analyses of patients with DNMT3A (n = 5) and IDH1/2 (n = 3) mutations should be considered exploratory given the extremely small sample sizes. These findings are hypothesis-generating rather than definitive and require validation in larger, multicenter cohorts.
Despite these limitations, our study provides clinically meaningful, real-world evidence in a frail elderly AML population that is often underrepresented in clinical trials. The results suggest that reduced-dose VEN combined with AZA may achieve durable remissions with manageable toxicity, while highlighting the need for prospective, multicenter studies with larger cohorts, longer follow-up, and incorporation of pharmacokinetic and QoL assessments to validate and extend these findings.





Comments (0)