In this observational study conducted at the Department of Gastroenterological Surgery, Osaka University, we evaluated the clinical efficacy of anamorelin in patients with gastric cancer-associated cachexia, successfully collecting data from 229 cases. Since the approval of anamorelin for the management of cancer cachexia, several clinical studies have investigated its efficacy. However, studies specifically focusing on patients with gastric cancer have been limited to post-marketing surveillance data provided by pharmaceutical companies, and to date, no detailed analyses of predictive factors influencing its efficacy have been reported [12,13,14,15,16]. In the present study, we demonstrated that oral administration of anamorelin in patients with gastric cancer-associated cachexia can be performed with relative safety. Moreover, a 12-week treatment period resulted in a significant and measurable increase in body weight. Notably, patients with lower baseline body mass index (BMI) exhibited a greater likelihood of achieving weight gain following treatment.
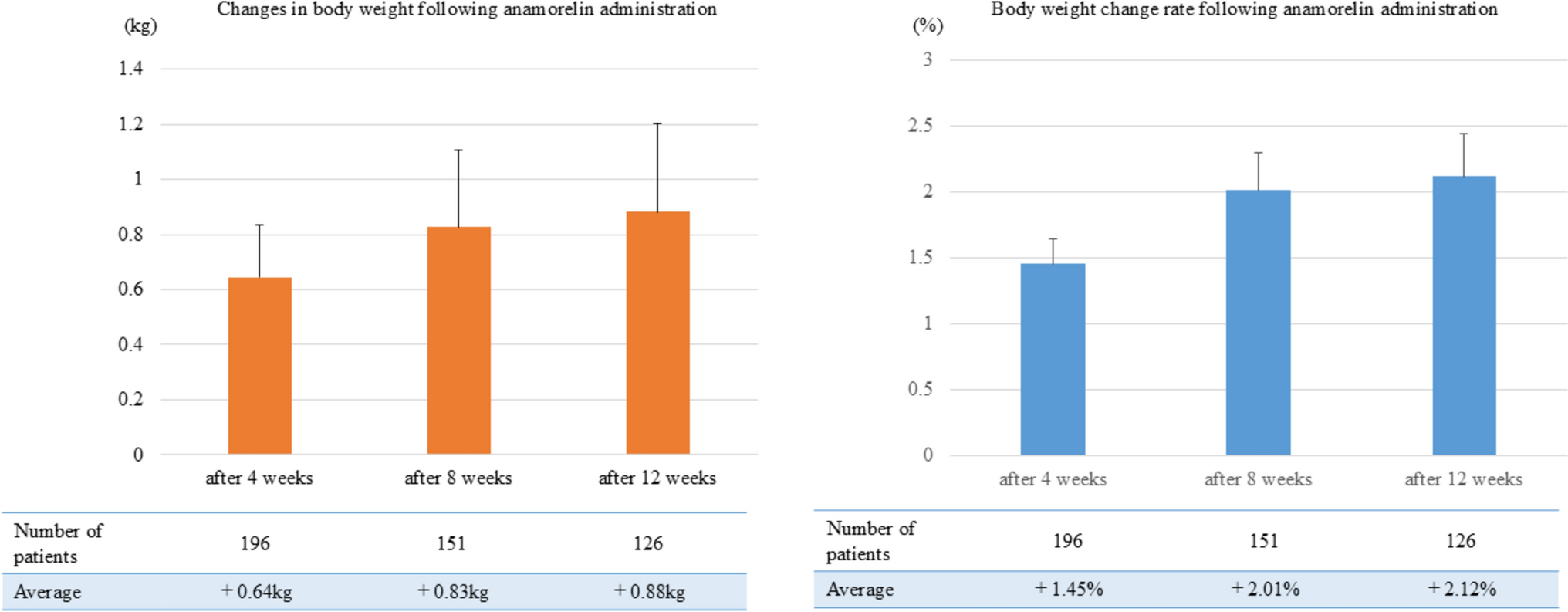
A previous postmarketing surveillance study reported a mean body weight gain of 1.1 kg following a 12-week course of anamorelin treatment [6]. Although that study included follow-up data for 1,076 patients with gastric cancer, only 294 patients had evaluable data at the 12-week time point, and the median duration of anamorelin administration was limited to 29 days. In contrast, in the present study, 126 of the 229 enrolled patients were successfully followed for 12 weeks, with a median treatment duration of 62 days and a mean body weight gain of 0.88 kg. Although direct comparisons between the two studies are inherently challenging due to differences in disease stage and treatment regimens, our findings demonstrated no clear association between improved treatment adherence and enhanced therapeutic benefits of anamorelin. These observations suggest that, in patients with gastric cancer-related cachexia, identifying predictive factors for anamorelin efficacy prior to treatment initiation may be of critical importance.
Although studies solely focusing on gastric cancer-related cachexia have not been conducted, several studies have investigated the efficacy of anamorelin in other malignancies, including pancreatic, colorectal, and non-small-cell lung cancers. Tsunematsu et al., in a study of 31 patients with pancreatic cancer, reported that a low CAR was a favorable predictive factor for the efficacy of anamorelin after 12 weeks [12]. Similarly, other studies involving patients with gastric, colorectal, pancreatic, and lung cancers have indicated that a lower mGPS, also based on serum CRP and albumin levels, was associated with a better treatment response [13, 14]. Moreover, Fujii et al. noted that patients with relatively preserved nutritional status, as indicated by a low Controlling Nutritional Status score calculated from serum albumin, total lymphocyte count, and total cholesterol levels, demonstrated significantly greater benefits from anamorelin across four cancer types for which anamorelin is approved for insurance coverage [15]. Although these studies included small sample sizes and diverse populations of patients with cancer, they collectively suggest that anamorelin can be more effective in patients who have not yet developed marked systemic inflammation or severe malnutrition. Consistent with these findings, our analysis revealed that patients with a high NLR, a systemic inflammation marker, were less likely to benefit from anamorelin, supporting the hypothesis that the systemic inflammatory burden may negatively affect the drug’s efficacy. In this study, mGPS and CAR—both calculated from serum albumin and CRP—were not identified as clear predictive markers of the efficacy of anamorelin. One possible explanation is that the eligibility criteria for anamorelin include albumin and CRP levels, and many patients in this cohort had abnormal values in these parameters at baseline, potentially attenuating the predictive utility of mGPS and CAR. Furthermore, hemoglobin levels ≥ 10 g/dL were identified as a significant factor associated with weight gain at 8 weeks after initiating anamorelin. Although no prior studies have reported a direct association between hemoglobin levels and the weight-increasing effect of anamorelin, previous literature has suggested that hemoglobin may be related to the progression and prognosis of cancer cachexia [7]. Furthermore, since hemoglobin reflects systemic status including nutritional condition, it is plausible that patients with hemoglobin ≥ 10 g/dL, indicating relatively preserved systemic condition, experienced greater weight gain. In patients with elevated systemic inflammation and malnutrition, the attenuated efficacy of anamorelin may be attributed, in part, to the underlying pathophysiological mechanisms. Cancer-related systemic inflammation activates pro-inflammatory cytokines, including interleukin (IL)-1, IL-6, and tumor necrosis factor alpha, which suppress appetite by acting on the hypothalamus and contribute to catabolic processes, including muscle degradation and lipolysis [17, 18]. These cytokines also disrupt ghrelin signaling, potentially weakening the appetite-stimulating effects of anamorelin [19]. Furthermore, the anabolic response to growth hormone and IGF-1 may be impaired by chronic inflammation, further limiting the efficacy of anamorelin in promoting weight or muscle gain [19]. Moreover, malnutrition and poor protein reserves may reduce the body’s capacity to respond to anabolic stimuli, further reducing the therapeutic potential of anamorelin.
Interestingly, the present study suggests that patients with a BMI of ≥ 20 kg/m2 were less likely to benefit from anamorelin. Although the median BMI in our cohort was 18.24 kg/m2, a subset of patients exhibited relatively higher BMI values. In these patients, baseline oral intake might have been sufficiently maintained, thereby limiting the appetite-stimulating effects of anamorelin. Notably, additional analyses of corporate clinical trial data related to the development of anamorelin have also reported greater efficacy in patients with BMI values below 20 kg/m2, which is consistent with the findings of our study [20]. To date, no studies have specifically identified an optimal BMI cutoff value for predicting the efficacy of anamorelin, and no established consensus currently exists. Nevertheless, early intervention during the pre-cachexia phase, prior to significant weight loss and malnutrition, is generally considered advantageous [7]. Based on the data from our study, a BMI of 20 kg/m2 may represent a potential threshold for selecting gastric cancer patients who are more likely to respond favorably to anamorelin therapy.
At the outset of this study, we hypothesized that patients who had undergone gastrectomy may derive greater benefits from anamorelin treatment than those with an intact stomach. This assumption was based on anamorelin’s mechanism of action as a ghrelin receptor agonist and the fact that circulating ghrelin levels are significantly decreased following gastrectomy [21]. Consequently, we expected that patients without a history of gastrectomy, who may demonstrate chronically elevated ghrelin levels due to cancer cachexia, would be less responsive to additional ghrelin receptor stimulation [22]. However, our findings showed that prior gastrectomy and body weight gain from anamorelin administration were not significant associated. Although this study did not measure serum ghrelin levels, previous studies have suggested that ghrelin levels can gradually recover over time in patients who had distal gastrectomy but not in those who underwent total gastrectomy [21]. This finding may partly explain the discrepancy between our hypothesis and the observed results. To clarify this issue, further prospective studies integrating serum ghrelin measurements are warranted.
This study had several limitations. First, we could not accurately evaluate skeletal muscle mass and muscle strength. Although the study protocol initially included plans to collect these data, performing it in the real-world clinical setting of an observational study involving patients with gastric cancer-related cachexia was challenging. Although previous clinical trials have reported that anamorelin increases skeletal muscle mass, no significant improvement in muscle strength was observed [2]. Therefore, future research focusing on the effects of anamorelin on muscle strength in patients with gastrointestinal cancer is needed. Furthermore, we attempted to collect data on nutritional markers such as rapid turnover proteins as surrogate indicators of skeletal muscle mass; however, the number of cases in which such data were available was too small to perform a reliable analysis. Second, as this study is an observational investigation involving gastric cancer patients treated with anamorelin, we were not able to perform a comparative analysis with a control group. To account for potential confounding factors inherent to this study design, we conducted multivariable analyses as a means of adjustment; however, we acknowledge that residual confounding may still exist. Furthermore, it is important to interpret the findings of this study in the context that anamorelin treatment was initiated based on the discretion of individual clinicians, and that a considerable proportion of patients were unable to complete 12 weeks of treatment, mainly due to disease progression. To address this, we are currently conducting a randomized controlled trial within our group to assess the efficacy of anamorelin in gastric cancer-related cachexia, and the results of that study are eagerly awaited. The last limitation of this study is that the analysis of treatment efficacy at 12 weeks after initiating anamorelin was restricted to patients who completed the 12-week follow-up. This factor should be taken into consideration when interpreting the study findings.
In conclusion, we analyzed 229 patients with gastric cancer-related cachexia who received anamorelin and confirmed that the treatment led to body weight gain. The NLR and BMI were identified as potential predictive factors for treatment efficacy. Active consideration of anamorelin therapy is warranted for patients likely to benefit from treatment, and clinical benefits beyond weight gain and skeletal muscle increase should be explored in future research.

Comments (0)