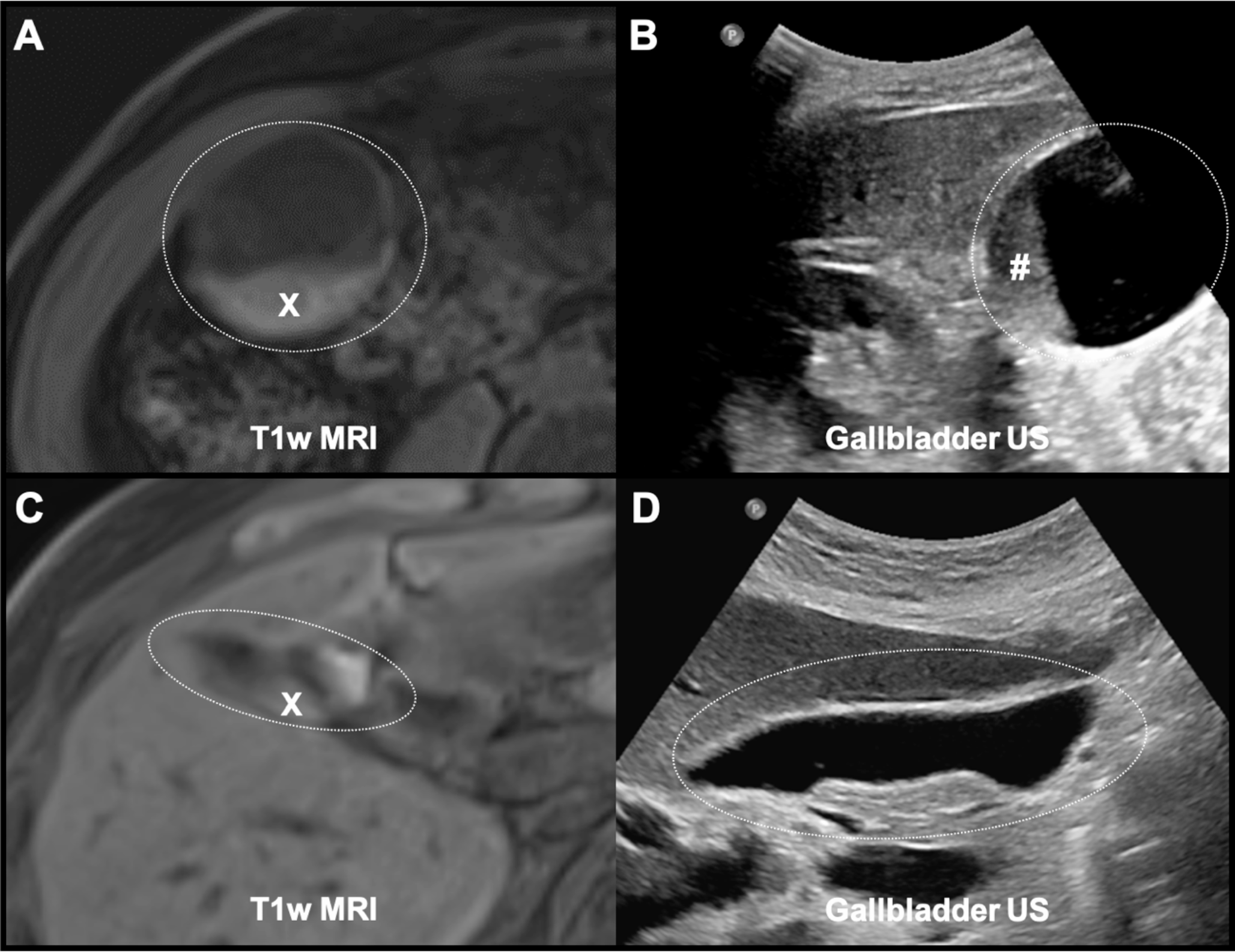
In this retrospective cohort and diagnostic accuracy study, we evaluated the clinical significance of T1w hyperintensity layering in the gallbladder and its predictive value for ultrasound-detected gallbladder sludge. Among the 415 patients with an established indication for abdominal imaging, T1w hyperintensity layering was observed in 56% of cases, with 54% of these patients demonstrating sludge on US. Notably, 92.7% of individuals with T1w layering were confirmed to have sludge in the US, underscoring a strong predictive association. These findings are consistent with previous reports [13] and reinforce the clinical relevance of T1w layering as a diagnostic marker.
T1w hyperintensity layering has been previously described in the literature, often attributed to the accumulation of mucus or proteinaceous material within the gallbladder, which may progress to sludge and eventually gallstone formation [12]. This phenomenon has been hypothesized as an early imaging biomarker for gallbladder pathology, offering the potential for timely clinical intervention [14]. While recent advancements in MRI techniques have enhanced the characterization of hepatobiliary disorders, the specific clinical implications of T1w layering remain uncertain [15]. Previous studies have suggested its association with chronic cholecystitis; however, others have struggled to link it to specific clinical symptoms, highlighting a gap that this study seeks to address [13, 16].
The findings of this study may contribute to the understanding of gallbladder pathology in patients with significant liver disease. Our results demonstrated that the presence of T1w layering detects gallbladder sludge with high sensitivity (92.7%). However, the moderate specificity (57.9%) necessitates cautious interpretation in clinical practice, as it may lead to false positives. This limitation highlights the importance of using T1w imaging in conjunction with other diagnostic modalities, such as ultrasound or T2-weighted imaging, to improve accuracy and reduce misdiagnosis. Previous studies have emphasized this multimodal approach as a strategy to enhance diagnostic reliability [17].
The layering phenomenon is thought to result from the accumulation of mucus or proteinaceous material, which can lead to sludge and ultimately gallstone formation. This suggests that T1w hyperintensity layering may serve as an early imaging biomarker for gallbladder pathology, potentially allowing for earlier clinical intervention. Comparatively, studies have shown varying results regarding the prevalence of sludge in liver disease patients, with some reporting a higher incidence in cirrhotic populations [10, 11]. It was highlighted that imaging features in hepatic and gallbladder pathologies might overlap, necessitating careful differentiation to avoid diagnostic inaccuracies [18]. In our cohort T1w layering was associated with the presence of sludge, thereby filling a gap in existing literature regarding imaging characteristics in this demographic. Our cohort predominantly consisted of patients with advanced liver disease, including conditions such as cirrhosis, portal hypertension, transjugular intrahepatic portosystemic shunt (TIPS) placement, and elevated liver function tests. This skewness toward significant liver pathology limits the generalizability of our findings to broader populations. Patients with hepatic dysfunction often exhibit alterations in the biliary milieu, which may predispose them to higher rates of gallbladder abnormalities, including sludge. Although these associations are supported by previous studies [16, 19], future research should prioritize diverse cohorts to evaluate whether similar correlations hold across varied clinical settings.
In addition to cholecystolithiasis (p < 0.001), elevated body mass index (BMI) was significantly associated with T1w layering in gallbladder sludge (p = 0.003). This finding may reflect altered bile composition, impaired gallbladder motility, and hormonal changes commonly observed in individuals with obesity. These findings are consistent with prior research [20, 21] and underscore the interplay between metabolic and biliary factors. However, other potential contributors, such as dietary habits and genetic predispositions, were not examined in this study. Future investigations should incorporate these variables to provide a more comprehensive understanding of biliary pathology [22, 23].
Interestingly, our study did not identify sex or age as significant predictors of gallbladder sludge, despite their well-established roles in gallstone formation [24]. This divergence from existing literature may reflect differences in the underlying mechanisms driving sludge versus gallstone development. The lack of association with markers of liver disease, such as cirrhosis, also warrants further investigation to delineate the specific pathophysiological processes influencing T1w layering.
The high prevalence of T1w hyperintensity layering and sludge in our cohort may, in part, be attributed to physiological bile hyperconcentration during non-per-oral (NPO) states. This finding aligns with previous studies suggesting that T1w layering may not always indicate pathology but instead reflect normal gallbladder dynamics [25, 26]. Distinguishing between physiological and pathological layering is critical to improving diagnostic specificity and preventing overdiagnosis. Future studies should focus on refining criteria to differentiate these phenomena.
Gallstone detection in our study was consistent with previously reported prevalence rates, with 24% of patients demonstrating gallstones on imaging. T1w imaging revealed also high sensitivity imaging for gallstone detection showing its valuable diagnostic role in settings where cost and accessibility are limiting factors [27, 28]. This reinforces the complementary role of T1w MRI alongside traditional imaging modalities, particularly in resource-constrained environments.
With an overall diagnostic accuracy of 77.3% and an area under the receiver operating characteristic (ROC) curve of 0.956, T1w layering emerges as a promising predictive marker, particularly for ruling out the absence of sludge. However, the moderate specificity necessitates a cautious approach, emphasizing the need for integration with clinical and laboratory data to enhance diagnostic confidence [29,30,31].
Despite the valuable findings of this study, several limitations must be acknowledged. As a single-center, retrospective study, the results are susceptible to selection bias and may not be generalizable to other populations. The lack of standardized follow-up and the potential for misinterpretation of physiologic bile hyperconcentration as pathologic cholestasis further limit the applicability of our results. Nevertheless, the homogeneity of data collection and analysis strengthens the internal validity of our findings.


Comments (0)