
Remember me





Antihypertensive therapy is key to the management of hypertension, with clinical guidelines recommending the use of multiple medicines to meet aggressive targets for blood pressure control [1]. People with hypertension often have multiple chronic conditions including coronary artery disease, diabetes, heart failure and chronic obstructive pulmonary disease; it is estimated that more than half have at least one additional comorbidity [2,3]. As such, people treated for hypertension often take a large number of medicines regularly [4,5], which can result in complex care pathways involving multiple health professionals.
Medicine adherence is fundamental to optimize treatment outcomes for hypertension, but can be challenging for people with complex care regimens [6]. Many opportunities exist for optimizing medicine use for patients with high medicine burden, such as medicine reviews and comprehensive medication management programs which review, identify and rectify medicine-related problems [7,8]. These opportunities reflect coordinated patient care across multiple providers within interdisciplinary teams such as primary care, specialist care and pharmacists [9]. In terms of chronic disease management, coordination of care can be achieved in different ways, such as through simplifying medicine administration or by streamlining the activities of prescribing and dispensing of medicines to consolidate healthcare interactions. These individual strategies for coordinating care in medicine management have been found to improve medicine adherence [10–12]. However, there is little evidence about the cumulative effect of employing multiple of these strategies. Hence, our aim was to assess the effects of multiple measures of coordinated care on adherence to antihypertensives among people using a large number of medicines.
METHODS Data sourceWe performed a retrospective cohort study using pharmaceutical claims data. Australia maintains a publicly funded, universal healthcare system entitling all citizens and permanent residents to subsidized medicines through the Pharmaceutical Benefits Scheme (PBS). PBS data captures information on PBS-listed medicines dispensed in community pharmacies, private hospitals, and on discharge from public hospitals in most states. We used PBS dispensing claims data from a randomly selected national sample of 10% of PBS-eligible people, provided by Services Australia, for the period 2017–2020 [13]. The PBS 10% sample contains the PBS item code, supply date, patient's year of birth, sex and year of death. We also used the PBS item code and PBS drug maps to obtain the generic name, pack size and format and strength of medicines dispensed. The PBS data are de-identified, but all records contain a unique person identification number that allows linkage of a person's records across multiple dispensing sites and prescribers. To protect privacy, all supply dates are offset by ±14 days and year of birth and death by ±180 days; this offset is the same for each individual [13].
CohortOur cohort included all adult (≥18 years) users of antihypertensive medicines between 1 July 2018 and 30 June 2019 (see Figure S1, Supplemental Digital Content, https://links.lww.com/HJH/C440 for more details of the study design). We chose these months so as to avoid irregular patterns of dispensing associated with end of year medicine stockpiling in the Australian PBS [13], and the potential disruptions to prescribing and dispensing associated with COVID-19. We identified users of first-line antihypertensives, including angiotensin-converting enzyme inhibitors (ACEi), angiotensin receptor blockers (ARB), calcium channel blockers (CCB), thiazide and thiazide-like diuretics and their fixed-dose combinations, identified using World Health Organization Anatomic Therapeutic Chemical (ATC) classification codes (Table S1, Supplemental Digital Content, https://links.lww.com/HJH/C440) [14]. We only included these medicine classes given other antihypertensives are commonly used for indications other than hypertension (e.g. beta blockers for myocardial infarction and heart failure). We identified the first observed dispensing of antihypertensives within the study period.
We restricted our cohort to people who were experiencing polypharmacy at the time of their first observed dispensing, defined as having dispensing of medicines for ≥5 unique active pharmaceutical ingredients in the prior 3 months. We excluded people whose date of death was on or before the first observed dispensing. As we did not have an exact date of death [13,15], we estimated the date of death as the last dispensing of any medicine within the potential range of the date of death [5].
We measured characteristics of our cohort as of the first observed dispensing, including age (in 18–49, 50–64, 65–74, 75–84 and ≥85 years age groups) and sex. We identified comorbidities using the Rx-Risk Comorbidity Index, using medicines dispensed in the 12 months prior to and including the first observed dispensing [16].
Coordinated careWe identified three measures reflective of processes in chronic disease management which could be used to coordinate the supply and administration of multiple medicines. These include: simple regimens in dose and form of antihypertensives and other cardiovascular medicines; continuity of prescribers; and coordination of medicine dispensing. Further details of each measure are in Tables S2–S4, Supplemental Digital Content, https://links.lww.com/HJH/C440. We measured all three measures of care within the 3 months before and including the date of the first observed dispensing of antihypertensive medicine [17].
Simple cardiovascular regimensWe measured the use of simple regimens (e.g. one pill a day) for each cardiovascular medicine [18]. To do this, we used the medication complexity score (MCS) [19] which includes components on both the dose forms (e.g. oral pills, sprays, injection pens) and daily dosing frequency (e.g. once daily, twice daily) of each medicine. The score begins at 2 (reflecting people taking their daily dose of every oral medicine in one pill), with a higher score indicating deviation from this pattern. We measured the average MCS across dispensings of cardiovascular medicines (including antihypertensives, lipid-lowering medicines, antiplatelets, anticoagulants, etc.; see Table S5, Supplemental Digital Content, https://links.lww.com/HJH/C440 for more details). We looked only at cardiovascular medicines because these are common therapies in people with hypertension [18], and often have similar potential patterns in utilization as antihypertensives. As the majority of cardiovascular medicines on the PBS are pills administered once daily, we therefore used an MCS of 2 to reflect having a simple cardiovascular regimen – as people taking their daily dose of each cardiovascular medicine as one oral pill.
Prescriber continuityWe measured prescriber continuity by examining the proportion of all medicine dispensings for a person prescribed by their most common prescriber. In line with similar measures of estimating continuity of care [20], we used a threshold for high continuity as having ≥0.75 of dispensings from a person's most common prescriber.
Dispensing coordinationWe measured dispensing coordination by examining the proportion of all medicines dispensed on the same day as one or more other medicine dispensing. This measure reflects the extent to which filling of prescriptions aligned with at least one other medicine, and does not require all prescriptions to be filled on the same day. Based on the distribution of the data (Figure S2, Supplemental Digital Content, https://links.lww.com/HJH/C440) and existing literature [17], we defined dispensing coordination using a threshold of ≥0.50.
Adherence to antihypertensivesWe estimated adherence using the proportion of days covered (PDC) from the date of first observed dispensing to death or 12 months, whichever occurred earlier. The PDC estimates the proportion of days that people have access to their medicine divided by the total follow-up period [21]. As daily dose information is not captured in our dataset, we assumed people used the minimum recommended dose for each antihypertensive medicine according to the Australian Medicines Handbook (see Table S6, Supplemental Digital Content, https://links.lww.com/HJH/C440 for details of estimated daily dose frequency). We verified this assumption by examining the median time between dispensings. We then divided the quantity dispensed by the daily dose information to obtain the duration of each dispensing. A covered date was defined as having at least one antihypertensive of interest on the date.
The calculation of PDC considered stockpiling and early refills. For people who had a subsequent dispensing of the same medicine before the previous dispensing ran out, this was carried forward and appended at the end of the previous dispensing. In addition, switches of medicines within the same medicine class (e.g., from captopril to enalapril) and between different medicine classes were allowed (e.g., from ACEi to ARB).
We defined a person as having high adherence if they achieve a PDC ≥0.8, which is a commonly used threshold associated with protective cardiovascular outcomes [22].
Statistical analysisWe used descriptive analyses to quantify the prevalence of the measures of coordinated care within our cohort. To explore independent associations between each measure of care and adherence to antihypertensives, we used unadjusted and adjusted (age, sex, number of comorbidities) logistic regression models. To determine if these associations were independent to the other measures of coordinated care, we then further included all three measures into a single adjusted (age, sex, number of comorbidities) model.
To explore the combined effect of multiple measures of coordinated care on adherence, we created a reparametrized variable reflecting each possible combination of the three measures of care. We included this variable in an age, sex and number of comorbidities adjusted logistic regression.
Associations between adherence and the measures of coordinated care were presented as odds ratios (ORs) with 95% confidence intervals (CIs). All data analyses were completed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA) and figures were produced using R version 4.3.1 (R Core Team 2017, Vienna, Austria).
Sensitivity analysesAs we have defined dichotomous measures of coordinated care, we also assessed the impact by treating each measure as a continuous variable. Prevalent users of antihypertensives may have a greater propensity to adhere to these medicines than new users, so we also performed a sensitivity analysis stratifying the cohort into new users, and prevalent users with 1–5 years or >5 years of prior use. We defined new users as those without any antihypertensive dispensing in the year prior to the beginning of the study period. We categorized prevalent users based on the number of consecutive years prior to the study period with at least one antihypertensive dispensing. As 47.5% of people were not experiencing polypharmacy at the time of first observed antihypertensive dispensing, we also assessed the impact of coordinated care on adherence in this cohort.
Ethics approval and data accessThe study was approved by the New South Wales Population and Health Services Research Ethics Committee (2019/ETH01176) with a waiver of individual consent. Data access was granted by the Services Australia External Request Evaluation Committee (RMS1941).
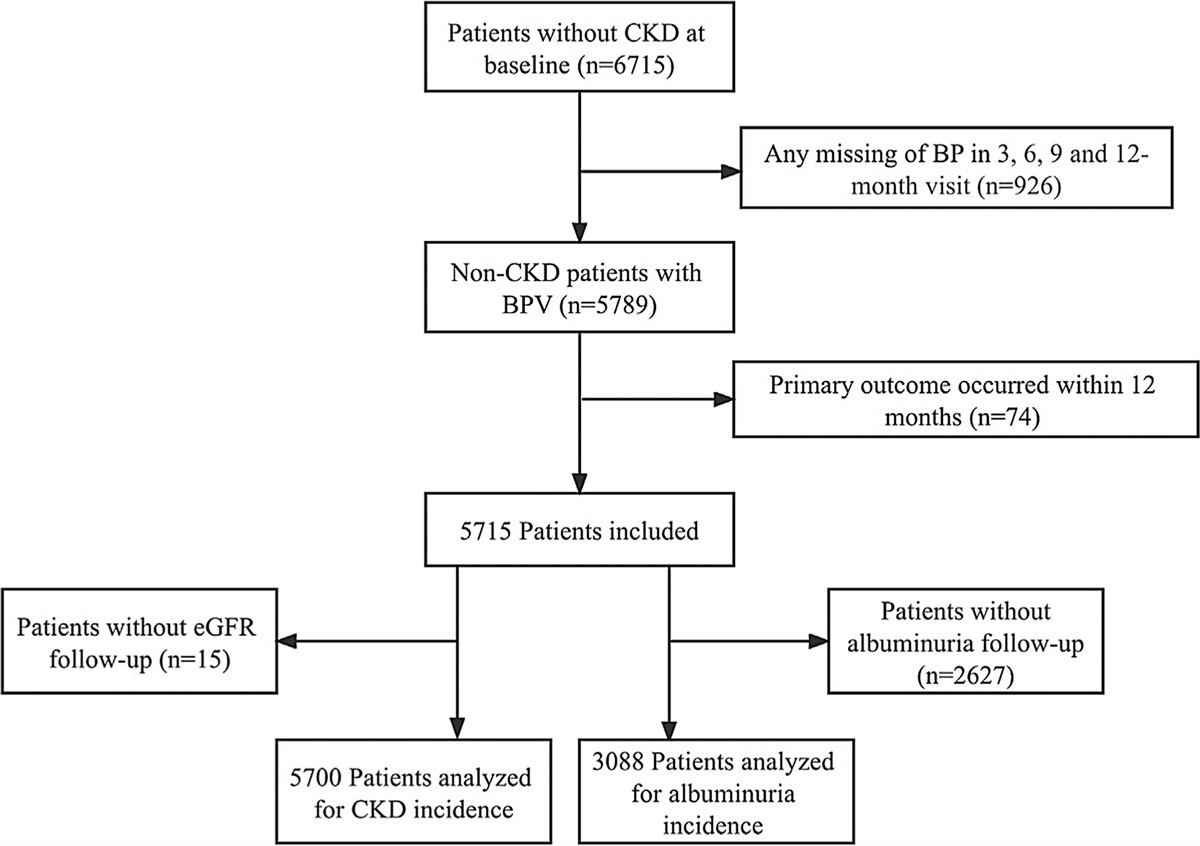
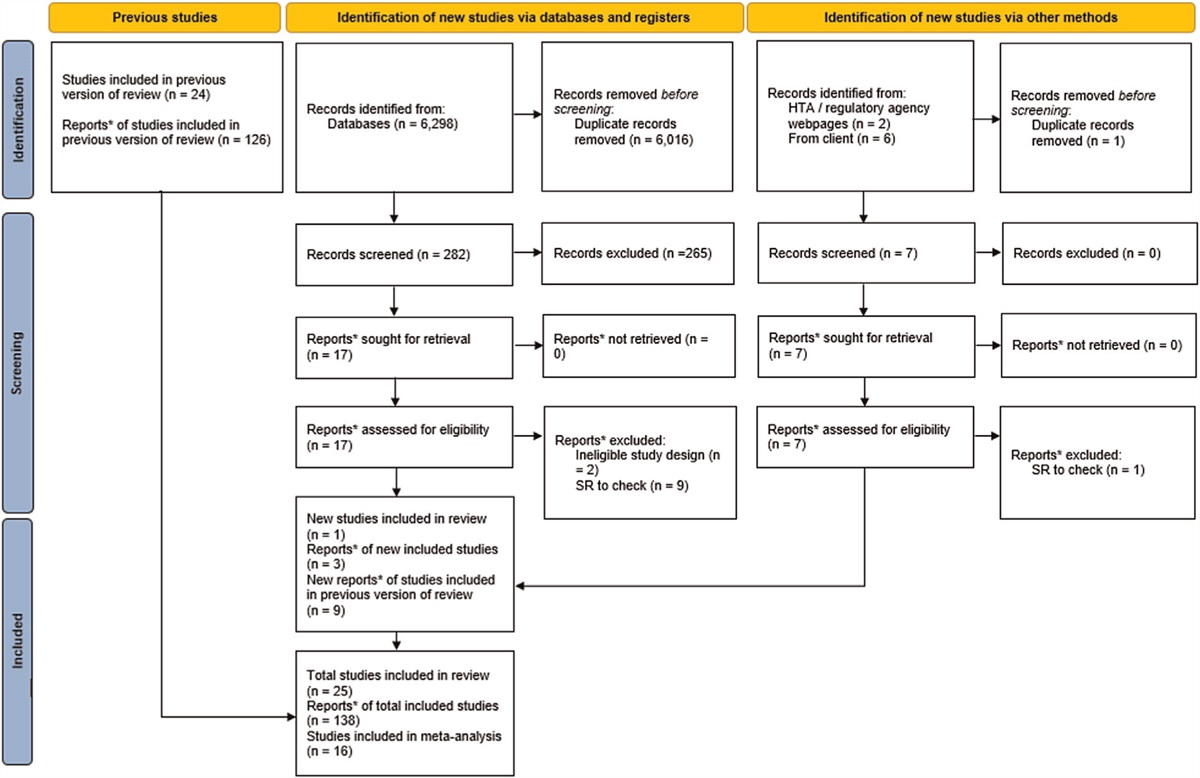
RESULTS Cohort characteristicsWe identified 387 839 adults who were alive and dispensed antihypertensive medicines between 1 July 2018 and 30 June 2019. Of these, 202 708 (52.3%) experienced polypharmacy in the prior 3 months and were included in our study (Fig. 1). The median age was 71 [interquartile range (IQR): 62–79] years, 48.9% were male, the median (IQR) number of active ingredients dispensed was 7 (6–10) and the median (IQR) number of comorbidities was 5 (4–7) (Table 1 and Figure S2, Supplemental Digital Content, https://links.lww.com/HJH/C440).
 FIGURE 1:
FIGURE 1: Diagram of cohort selection.
TABLE 1 - Characteristics of antihypertensive users experiencing polypharmacy at the time of their first observed antihypertensive dispensing Characteristics N (% of total) Total number of people 202 708 (100.0) Age group (years) 18–49 13 260 (6.5) 50–64 49 853 (24.6) 65–74 63 811 (31.5) 75–84 53 363 (26.3) ≥85 22 421 (11.1) Sex Female 103 656 (51.1) Male 99 052 (48.9) Number of comorbiditiesa 1–2 10 156 (5.0) 3–5 101 745 (50.2) >5 90 807 (44.8) Type of first observed antihypertensive Angiotensin-converting enzyme inhibitors (ACEi) 52 504 (25.9) Angiotensin receptor blockers (ARB) 52 731 (26.0) Calcium channel blockers (CCB) 28 999 (14.3) Thiazide and thiazide-like diuretics (TD) 1327 (0.7) Fixed-dose combinations 67 147 (33.1) ACEi + CCB 12 696 (6.3) ACEi + TD 5673 (2.8) ARB + CCB 11 038 (5.4) ARB + TD 27 578 (13.6) ARB + CCB + TD 5933 (2.9) CCB + lipid lowering agents 4229 (2.1) Cardiovascular medicines dispensed within prior 3 months Angiotensin-converting enzyme inhibitors 80 108 (39.5) Angiotensin receptor blockers 111 436 (55.0) Calcium channel blockers 88 476 (43.6) Thiazide and thiazide-like diuretics 50 774 (25.0) Lipid lowering agents 133 222 (65.7) Anticoagulants 28 578 (14.1) Antiplatelets 23 428 (11.6) Beta-blockers 57 732 (28.5) Other cardiovascular medicines 48 069 (23.7) Number of unique cardiovascular medicines dispensed within the prior 3 months 1 33 769 (16.7) 2 61 790 (30.5) 3 48 464 (23.9) 4 31 153 (15.4) ≥5 27 532 (13.7) Measures of coordinated care Simple cardiovascular regimens 133 707 (66.0) Prescriber continuity 128 222 (63.3) Dispensing coordination 132 791 (65.5) Multiple measures of coordinated care None of the above 8878 (4.4) 1 of the above 50 511 (24.9) 2 of the above 85 748 (42.4) 3 of the above 57 571 (28.4)aThis was derived from the Rx-Risk Comorbidity Index.
The most common antihypertensives of the first observed dispensing were ARBs (48.0%). Approximately one-third of people (33.1%) had a fixed-dose combination for their first observed dispensing, and the most common combination was ARB and thiazide and thiazide-like diuretics (13.6%) (Table 1). Most people were prevalent users of antihypertensives, with the majority (85.9%) having a prior dispensing of an antihypertensive within the 3 months prior to the first observed dispensing within the study period. One-sixth of people were dispensed one unique cardiovascular medicine (16.7%), one-third were dispensed two (30.5%), and about half of them were dispensed at least three unique cardiovascular medicines within the prior 3 months (53.0%). A total of 5425 (2.7%) people died within one year of follow-up.
Coordinated care 3-months prior to and including the first observed antihypertensive dispensingApproximately two-thirds of people (66.0%) had simple cardiovascular regimens, meaning they were taking their daily dose of all cardiovascular medicines each as one oral pill (Table 1). For the other third of people, their cardiovascular medicines differed mostly from people using more than one oral pill for at least one of their cardiovascular medicines. The median (IQR) average cardiovascular MCS was 2.0 (2.0–2.3) (Figure S2, Supplemental Digital Content, https://links.lww.com/HJH/C440).
Approximately two-thirds of people (63.3%) experienced prescriber continuity, meaning that the majority (more than 75%) of them had more than 75% of their medicine dispensings being prescribed from their single most common prescriber (Table 1). The median (IQR) proportion of dispensings from the most common prescriber was 0.8 (0.6–1.0) (Figure S2, Supplemental Digital Content, https://links.lww.com/HJH/C440).
Approximately two-thirds of people (65.5%) experienced dispensing coordination, meaning that over 50% of all their medicine dispensings occurred on the same day as at least one other dispensing (Table 1). The median (IQR) proportion of medicines dispensed on same day as another was 0.6 (0.4–0.7) (Figure S2, Supplemental Digital Content, https://links.lww.com/HJH/C440).
Almost a third (28.4%) of people experienced all three measures of coordinated care, 42.4% experienced two of the three, 24.9% experienced only one, and 4.4% did not experience any of these measures of care (Table 1 and Fig. 2).
 FIGURE 2:
FIGURE 2: Prevalence of measures of coordinated care.
Impact of each measure of coordinated care on adherence to antihypertensivesOverall, 78.9% (N = 159 847) of people were considered to have high adherence (PDC ≥ 0.8); with a median (IQR) PDC of 1.0 (0.8–1.0). Although the use of simple cardiovascular regimens was associated with decreased adherence in the unadjusted model (OR = 0.97, 95% CI: 0.95–0.99), it was marginally associated with increased adherence after adjusting for age, sex and number of comorbidities (adjusted OR = 1.06, 95% CI: 1.04–1.09) (Table 2). Both prescriber continuity (adjusted OR = 1.31, 95% CI: 1.28–1.34) and dispensing coordination (adjusted OR = 1.21, 95% CI: 1.19–1.24), were associated with increased adherence in both the unadjusted as well as the age, sex and number of comorbidities adjusted models. These adjusted associations remained when fully adjusting by the other measures of coordinated care (Table 2).
TABLE 2 - Associations between each measure of coordinated care with adherence (proportion of days covered ≥0.8) to antihypertensives Coordinated care No. people AdherentCI, confidence interval; OR, odds ratio.
aAdjusted for age group, sex, number of comorbidities and the other measures of coordinated care.
We observed an increasing trend in adherence with the number of measures of coordinated care (Fig. 3). The highest adherence (adjusted OR = 1.63) was observed among people experiencing all three measures. Similarly, adherence tended to be higher among those experiencing two measures (adjusted OR range of 1.33–1.47) and one measure (OR range of 1.02–1.43) compared with those not experiencing any measure of coordinated care (Fig. 3). Combinations involving prescriber continuity and/or dispensing coordination were consistently associated with higher adherence; with ORs ranging from 1.20 to 1.63 (Fig. 3). The only statistically significant associations for simple cardiovascular regimens were when it was concurrent with prescriber continuity and/or dispensing coordination.
 FIGURE 3:
FIGURE 3: Associations between multiple measures of coordinated care with adherence (proportion of days covered ≥0.8) to antihypertensives.
Sensitivity analysesWhen treating each measure of coordinated care as a continuous variable, we found similar patterns of association of each measure of care and adherence (Table S7, Supplemental Digital Content, https://links.lww.com/HJH/C440).
The majority of our cohort were prevalent users of antihypertensives (n = 43 493 in people with 1–5 years; n = 144 142 in those with >5 years); approximately 7.4% were new users. Adherence tended to be lowest in new users (45.8% with PDC ≥ 0.8) and higher in prevalent users (70.6% in people with 1–5 years; 84.8% in people with >5 years respectively). When stratifying by prior antihypertensive use, we did not observe significant associations between measures of coordinated care and adherence among new users. However, we did observe broadly similar patterns of association among groups of prevalent users as with the main analysis (Figure S3, Supplemental Digital Content, https://links.lww.com/HJH/C440).
In our study cohort of antihypertensive users who were not experiencing polypharmacy (N = 184 353; Fig. 1), we found slightly different patterns of coordinated care, with higher proportions of simple cardiovascular regimens and prescriber continuity but a lower proportion of dispensing coordination, than our main analysis (Table S8, Supplemental Digital Content, https://links.lww.com/HJH/C440 and Figure S4, Supplemental Digital Content, https://links.lww.com/HJH/C440). We also found a lower rate of adherence (69.5%). We similarly found that prescriber continuity and dispensing coordination alone or in combination were associated with increased adherence, but did not observe a pattern of increasing adherence with a higher number of measures of coordinated care (Figure S5, Supplemental Digital Content, https://links.lww.com/HJH/C440).
DISCUSSIONOur study found that prescribing and dispensing activities reflecting coordination of care were associated with increased adherence to antihypertensive medicines. This effect was strongest in people experiencing multiple measures of coordination, particularly prescriber continuity with dispensing coordination. These results highlight that while there may be multiple strategies for enhancing medicine management for cardiovascular disease and its related high-risk factors, the benefit of adherence may be in utilizing comprehensive strategies which coordinate both prescribing and dispensing of both cardiovascular and noncardiovascular medicines.
Our findings support the development of strategies to optimize prescribing and dispensing activities on hypertension management, which is a priority of governments in Australia and worldwide [6,23]. In clinical practice, strategies for integrated care aiming to coordinate prescribing activities, such as comprehensive medication management [7] and medicine reviews [8], have demonstrated significant effects in enhancing medicine adherence. These approaches often involve a multidisciplinary team of healthcare professionals, such as general practitioners (GPs), specialists and pharmacists, working together to optimize a patient's medicine regimen [7]. This collaborative effort includes activities such as medicine reconciliation, identification of potential drug interactions or adverse effects, dosage adjustments and patient education [24,25], and has been found to lead to significant improvements in adherence [26,27]. Our findings that people with coordination of both their prescribing and dispensing of medicines tended to have the highest adherence is supportive of strategies which foster increased collaboration between GPs, specialists and pharmacists in medicine management.
Our findings show relatively modest benefits in use of a simplified regimen of cardiovascular medicines; while there is an overall association, this appears to be driven by the large proportion of people who concurrently experience coordination of both prescribing and dispensing. While this suggests there is greater benefit in integration of care across the health system than in convenience of administration, the benefits of a simplified administration should not be dismissed. For example, polypills which combine multiple active ingredients on the same pill have an additional benefit in synchronizing prescribing and dispensing of multiple medicines [28]. Such people experiencing all three forms of coordinated care had the highest rates of adherence within our study.
Although activities such as comprehensive medication management and Medicine Reviews are often targeted towards people experiencing polypharmacy, we similarly found patterns of higher adherence with coordinated care in people using <5 medicines. It is harder to assess such associations when people are using fewer medicines, but the relatively large effect sizes suggest there are significant benefits of prescriber continuity and harmonization of dispensing on adherence to antihypertensives.
To the best of our knowledge, this is the first study to examine the cumulative effect of employing multiple strategies in combination on adherence to cardiovascular medicines using large-scale observational data. While few studies have explored multiple strategies for which we can compare our results, our findings in relation to the individual strategies were consistent with prior research [11,12,29–32]. Multiple systematic reviews have found that simple regimens (e.g. once-daily administration) are associated with higher adherence to therapy than those with more (e.g. twice-daily or thrice-daily) for a range of chronic conditions – with an increase of adherence ranging from 13.1% to 44.0% [29,30,32]. Similarly, compared to complex dosing forms (e.g. spays, injection pens), simple dosing forms such as oral pills are associated with higher adherence [30].
Fewer studies have investigated the effects of prescriber continuity. Adherence to antihypertensive and antidyslipidemia medicines have been found to be significantly lower in patients seeing multiple prescribers than those with one prescriber of these medicines (ORs of 0.69, 0.86 respectively) [11]. Similarly, higher continuity of care in GP consultations has been found to be associated with a 5% increase in statin adherence [31]. While we could not identify observational studies exploring the effect of dispensing coordination on adherence, a meta-analysis of medicine synchronization programs that coordinate medicine refills to a single day or pharmacy visit found a more than two-fold increase of adherence (pooled OR of 2.29, 95% CI: 1.99–2.64) [12].
There are many factors across the care continuum which influence both care coordination and medicine adherence, and there remains potential for confounding. For example, the majority of our cohort were prevalent users – who may be disposed to higher adherence. Although our sensitivity analysis found similar patterns of association in prevalent users with different durations of therapy (and levels of adherence), we did not find any associations among new users. Prior studies have similarly found the benefits of fixed-dose combination therapies on adherence among prevalent users only [33], and it may be that the benefits of coordinated care are in people with established long-term treatment. The role of health on adherence to medicines is complex, for example older people with more comorbidities have been reported to have higher rates of adherence [31], yet are also those most likely to be the focus of deprescribing initiatives. While our study adjusted for comorbidities, we were unable to capture treatment decisions around the medication burden which could have influenced our measure of adherence.
Several limitations should be considered. First, as there is no information available on daily doses and we used the minimum recommended dose by the Australian Medicines Handbook to estimate the dose frequency of the MCS as well as to attribute treatment duration, we may have underestimated the estimation of medication complexity score and overestimated adherence. However, most cardiovascular medicines included are usually taken once daily, and our duration proxy was verified and modified by examining the median time between dispensings, so the potential for bias is expected to be small. Second, as the PBS claims data do not capture private and public hospital inpatient prescriptions, adherence may be underestimated. Third, we are assessing coordinated care and adherence in different exposure and follow-up periods, and there may be further changes in patients’ care between these which may impact adherence. However, the majority of our cohort (92.6%) were prevalent users of antihypertensive medicines who tend to have more stable care. Fourth, we had limited measures of care coordination, and were unable to assess, for example, simplified regimen of all medications. While our focus on dose form and frequency of cardiovascular medicines reflects prescribing patterns likely to occur with the same prescriber as antihypertensives, it is possible that people using large numbers of noncardiovascular medicines will potentially have complicated care pathways and administration. Finally, while we used dichotomous measures in our study, there are likely to be a continuum over which coordination of either prescribing or dispensing is likely to impact adherence. Similarly, while adherence is commonly measured using a threshold of ≥0.8, benefits of antihypertensive therapy may also be reached with lower thresholds of adherence. Although the results of our sensitivity analysis using continuous variables were broadly consistent with our main analysis, further work identifying optimal pathways of coordinated care can help inform future strategies of improving adherence.
CONCLUSIONCoordinated care in people using antihypertensive medicines can help improve adherence, particularly when combining multiple strategies to consolidate both prescribing and supply of patients’ medicines. These benefits are cumulative, supporting comprehensive and collaborative medicine management strategies for both cardiovascular and noncardiovascular medicines.
ACKNOWLEDGEMENTSWe acknowledge Melisa Litchfield for her role in providing the data and gaining ethics approval. We thank the Australian Government Services Australia for supplying the data.
Sources of funding: This research is supported by the National Health and Medical Research Council (NHMRC) Ideas Grants (grant number: 2002889; grant number: 1183273) and NHMRC Medicines Intelligence Centre of Research Excellence (grant number: 1196900). MOF is supported by a Future Leader Fellowship from the National Heart Foundation of Australia (grant number: 105609). AES is supported by a NHMRC Leadership Investigator Grant (grant number: 2017504).
Disclosures: S.A.P. is a member of the Drug Utilisation Sub Committee of the Pharmaceutical Benefits Advisory Committee. The views expressed in this paper do not represent those of the Committee.
Conflicts of interestThere are no conflicts of interest.
REFERENCES 1. Hoare E, Kingwell BA, Jennings GLR. Blood pressure down under, but down under what? US and Australian Hypertension Guideline Conversation. Hypertension 2018; 71:972–975. 2. Barnett K, Mercer SW, Norbury M, Watt G, Wyke S, Guthrie B. Epidemiology of multimorbidity and implications for healthcare, research, and medical education: a cross-sectional study. Lancet 2012; 380:37–43. 3. Tran JA-O, Norton RA-OX, Canoy DA-O, Ayala Solares JA-O, Conrad NA-O, Nazarzadeh MA-O, et al. Multimorbidity and blood pressure trajectories in hypertensive patients: a multiple landmark cohort study. PLoS Med 2021; 18:e1003674. 4. Walsh CA, Cahir C, Bennett KE. Association between adherence to antihypertensive medications and health outcomes in middle and older aged community dwelling adults; results from the Irish longitudinal study on ageing. Eur J Clin Pharmacol 2019; 75:1283–1292. 5. de Oliveira Costa J, Lin J, Pearson S-A, Buckley NA, Schaffer AL, Falster MO. Persistence and adherence to cardiovascular medicines in Australia. J Am Heart Assoc 2023; 12:e030264. 6. Burnier M, Egan BM. Adherence in hypertension. Circ Res 2019; 124:1124–1140. 7. Pharmaceutical Society of Australia. Guidelines for comprehensive medication management reviews. 2020; Available at: https://my.psa.org.au/s/article/guidelines-for-comprehensive-mmr. 8. Blenkinsopp A, Bond C, Raynor DK. Medication reviews. Br J Clin Pharmacol 2012; 74:573–580. 9. World Health Organisation. Continuity and coordination of care. 2018; Available at: https://iris.who.int/bitstream/handle/10665/274628/9789241514033-eng.pdf?isAllowed=y&sequence=1. 10. Whelton PK, Williams B. The 2018 European Society of Cardiology/European Society of Hypertension and 2017 American College of Cardiology/American Heart Association Blood Pressure Guidelines: more similar than different. JAMA 2018; 320:1749–1750. 11. Hansen RA, Voils CI, Farley JF, Powers BJ, Sanders LL, Sleath B, et al. Prescriber continuity and medication adherence for complex patients. Ann Pharmacother 2015; 49:293–302. 12. Nsiah I, Imeri H, Jones AC, Bentley JP, Barnard M, Kang M. The impact of medication synchronization programs on medication adherence: a meta-analysis. J Am Pharm Assoc 2021; 61:e202–e211. 13. Mellish L, Karanges EA, Litchfield MJ, Schaffer AL, Blanch B, Daniels BJ, et al. The Australian Pharmaceutical Benefits Scheme data collection: a practical guide for researchers. BMC Res Notes 2015; 8:634. 14. Gabb GM, Mangoni AA, Anderson CS, Cowley D, Dowden JS, Golledge J, et al. Guideline for the diagnosis and management of hypertension in adults – 2016. Med J Aust 2016; 205:85–89. 15. Mealing NM, Dobbins TA, Pearson SA. Validation and application of a death proxy in adult cancer patients. Pharmacoepidemiol Drug Saf 2012; 21:742–748. 16. Pratt NL, Kerr M, Barratt JD, Kemp-Casey A, Kalisch Ellett LM, Ramsay E, et al. The validity of the Rx-Risk Comorbidity Index using medicines mapped to the Anatomical Therapeutic Chemical (ATC) Classification System. BMJ Open 2018; 8:e021122. 17. Choudhry NK, Fischer MA, Avorn J, Liberman JN, Schneeweiss S, Pakes J, et al. The implications of therapeutic complexity on adherence to cardiovascular medications. Arch Intern Med 2011; 171:814–822. 18. Schaffer AL, Chia J, Brett J, Pearson S-A, Falster MO. A nationwide study of multimedicine use in people treated with cardiovascular medicines in Australia. Pharmacotherapy 2022; 42:828–836. 19. Kitchen CA, Chang HY, Bishop MA, Shermock KM, Kharrazi H, Weiner JP. Comparing and validating medication complexity from insurance claims against electronic health records. J Manag Care Spec Pharm 2022; 28:473–484. 20. Tran B, Falster M, Jorm L. Claims-based measures of continuity of care have nonlinear associations with health: data linkage study. Int J Popul Data Sci 2018; 3:463. 21. Leslie SR, Gwadry-Sridhar F, Thiebaud P, Patel BV. Calculating medication compliance, adherence and persistence in administrative pharmacy claims databases. Pharma Program 2008; 1:13–19. 22. De Vera MA, Bhole V, Burns LC, Lacaille D. Impact of statin adherence on cardiovascular disease and mortality outcomes: a systematic review. Br J Clin Pharmacol 2014; 78:684–698. 23. Schutte AE, Webster R, Jennings G, Schlaich MP. Uncontrolled blood pressure in Australia: a call to action. Med J Aust 2022; 216:61–63. 24. Westberg SM, Derr SK, Weinhandl ED, Adam TJ, Brummel AR, Lahti J, et al. Drug therapy problems identified by pharmacists through comprehensive medication management following hospital discharge. J Pharm Tec
Comments (0)