
Remember me





Uncontrolled arterial hypertension is a leading risk factor for serious cardiovascular complications, such as stroke, coronary artery disease and heart failure, as well as severe kidney damage [1]. Uncontrolled hypertension is considered ‘treatment-resistant’ when blood pressure (BP) remains above 140/90 mmHg despite recommended lifestyle changes and the use of three classes of antihypertensive medication, including a diuretic [2,3].
Renal denervation (RDN) is a minimally invasive, catheter-based procedure that ablates the sympathetic nerves adjacent to the renal artery walls. This reduces the sympathetic efferent signalling to, and sensory afferent signalling from, the kidneys [4,5] and has been shown to reduce BP [6]. RDN is recommended for the treatment of hypertension in the 2023 European Society of Hypertension Guidelines [3] and has been approved by the United States Food and Drug Administration for clinical use in patients with uncontrolled hypertension [7].
Existing systematic reviews and meta-analyses investigating RDN [6,8–14] do not include the results of two pivotal, double-blind, sham-controlled trials (RADIANCE II [15] and the SPYRAL HTN-ON MED expansion [16]) that were published in 2023. These are essential to a contemporary understanding of the field and were conducted according to the standards laid out in the European Society of Cardiology (ESC)/European Association of Percutaneous Cardiovascular Interventions (EAPCI) and the Hypertension Academic Research Consortium (HARC) consensus statements [17].
Previous systematic reviews and meta-analyses suggest that RDN consistently reduces BP throughout a 24 h window, which could prove important in the management of patients as it addresses patient nonadherence or intolerance to antihypertensive drugs [8,9]. A further reason for the current analysis is that, whilst prior meta-analyses have been conducted, methodological disparities between the systematic reviews and trials included make conclusions difficult to generalize. These disparities include differences in the consideration and analysis of trial populations, comparator arms, and outcomes assessed.
The current systematic review and meta-analysis was undertaken according to the principles in the Cochrane Handbook and aims to comprehensively examine the randomized controlled trial (RCT) evidence for radiofrequency and ultrasound RDN in comparison with antihypertensive medication, a sham procedure, or another RDN modality in patients with uncontrolled arterial hypertension. Important subgroups, including treatment-resistant hypertension, were considered.
SYSTEMATIC REVIEW METHODSThe systematic review was undertaken according to the principles published in the Cochrane Handbook[18] and guidance published by the Centre for Reviews and Dissemination [19]. A protocol to inform the systematic review was developed a priori and registered on the PROSPERO database (CRD42022374189) [20].
Review eligibility criteriaRCTs of any duration that included patients with uncontrolled hypertension, aged 18 years or older, were eligible. The focus on RCTs was selected because of the lower risk of methodological bias and rigorous design [18]. Uncontrolled hypertension was defined by an office SBP or DBP of greater than or equal to 140 or 90 mmHg, respectively. Trials were included if they assessed a radiofrequency and/or ultrasound, catheter-based RDN procedure compared with antihypertensive drug treatment, sham procedure, or another RDN modality. Eligible RCTs were those that concomitantly used antihypertensive medication (of any class) [3] or were treatment-naive at baseline. Outcomes for the meta-analysis were prioritized as follows:
1. BP outcomes: a. Change from baseline in office SBP or DBP b. Change from baseline in ambulatory (24-h) SBP or DBP c. Change from baseline in day and night-time ambulatory BP 2. Safety outcomes: a. Serious adverse eventsOther eligible outcomes included changes in antihypertensive medication and medication adherence. Supplemental Digital Content 1 Appendix A, https://links.lww.com/HJH/C452 presents the full eligibility criteria.
Identification and selection of relevant studiesA MEDLINE (OvidSP) search strategy was designed comprising three concepts: hypertension AND renal denervation AND RCTs. The search strategy was not restricted by language or date. Six databases, two trial registers and three health technology assessment/regulatory agency webpages were searched (Supplemental Digital Content 1 Appendix B, https://links.lww.com/HJH/C452). The full search strategies can be found in Supplemental Digital Content 1 Appendix C, https://links.lww.com/HJH/C452.
Two reviewers (A.L.S. and J.P.) independently assessed the identified records for relevance against the review eligibility criteria. Disagreements were resolved by a third reviewer. Titles and abstracts of the records were assessed first, followed by the full text paper of any potentially relevant trials. The number of records included and excluded at each stage of the study selection process were recorded in a PRISMA flow diagram [21,22].
Data extraction and risk of bias assessmentThe data were extracted into a structured extraction template in Microsoft Excel. Data extraction and risk of bias assessments were undertaken by one reviewer (J.P.), with a second reviewer (A.L.S.) checking all data points. Any discrepancies were resolved by a third reviewer. The extracted data elements included trial methodology, patient characteristics, intervention details, details of any statistical analysis, and the eligible outcome data. Outcome data was collected for all timepoints reported. The Cochrane Risk of Bias 2 tool was used to critically appraise the RCTs [23].
Feasibility assessmentA qualitative feasibility assessment was conducted to assess the similarity of the RCTs identified in the systematic review. This assessed trial characteristics (including location, setting and follow-up), patient characteristics (including baseline antihypertensive medication and adherence), interventions and comparators, and outcomes (including outcome definitions and timepoints of assessment). Trials that were suitably similar were considered for meta-analysis. The feasibility assessment was conducted based on guidance produced by the Australian Pharmaceutical Benefits Advisory Committee [24].
Meta-analysisA meta-analysis was conducted for groups of trials that were considered comparable by the feasibility assessment. In order to be included in the meta-analysis, the trials must have reported sufficient data (mean or median with a measure of uncertainty reported) to inform the analysis. 95% confidence intervals or standard errors were converted to standard deviation prior to inclusion in the meta-analysis.
Trial data were pooled and analysed using both a fixed effect and a random effect model to estimate the mean differences for continuous outcomes and risk ratios (RRs) for binary outcomes. Supplemental Digital Content 1 Appendix D, https://links.lww.com/HJH/C452 contains details on the statistical methods applied. The sensitivity of the results to potential outliers and potential sources of heterogeneity were evaluated through sensitivity analyses. All statistical analyses were conducted using R version 4.2.1 [25]. The following R packages were also used: tidvverse (v.1.3.2) [26], meta (v.6.0.0) [27], metafor (v.3.8.1) [28] and dmetar (v.0.0.9000) [29]. All results were displayed on a forest plot and significance was defined as P ≤ 0.05.
Subgroup and sensitivity analysisA total of four subgroups were predefined and had sufficient data to inform a meta-analysis: resistant hypertension (defined for this analysis as patients on ≥3 medications, with or without a diuretic), radiofrequency-only trials, ultrasound-only trials and second-generation-only trials. There were insufficient data to inform planned subgroup analysis of patients with comorbidities and with differing baseline BP.
Sensitivity analyses were conducted to assess the robustness of the base case analysis. They assessed the impact of outliers, of limiting RCTs to sham only, or of RCTs meeting the quality criteria defined by the ESC/EAPCI consensus statement (i.e. second-generation sham RCTs with medication adherence measurement and blinding of outcome assessment) [30], and evaluated the treatment effect of radiofrequency devices only in the treatment-resistant subgroup.
The trials included in the meta-analysis and subgroup analyses for each outcome are reported in Supplemental Digital Content 1 Appendix E, https://links.lww.com/HJH/C452.
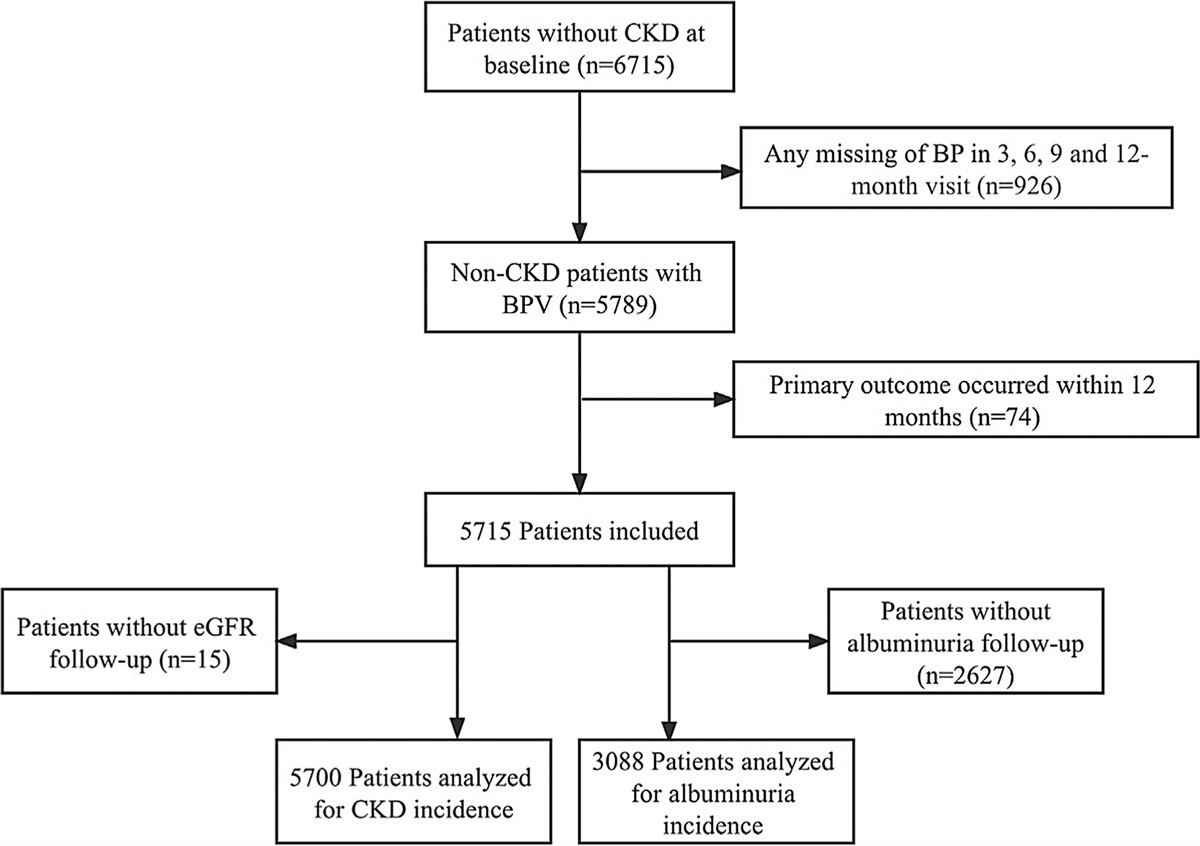
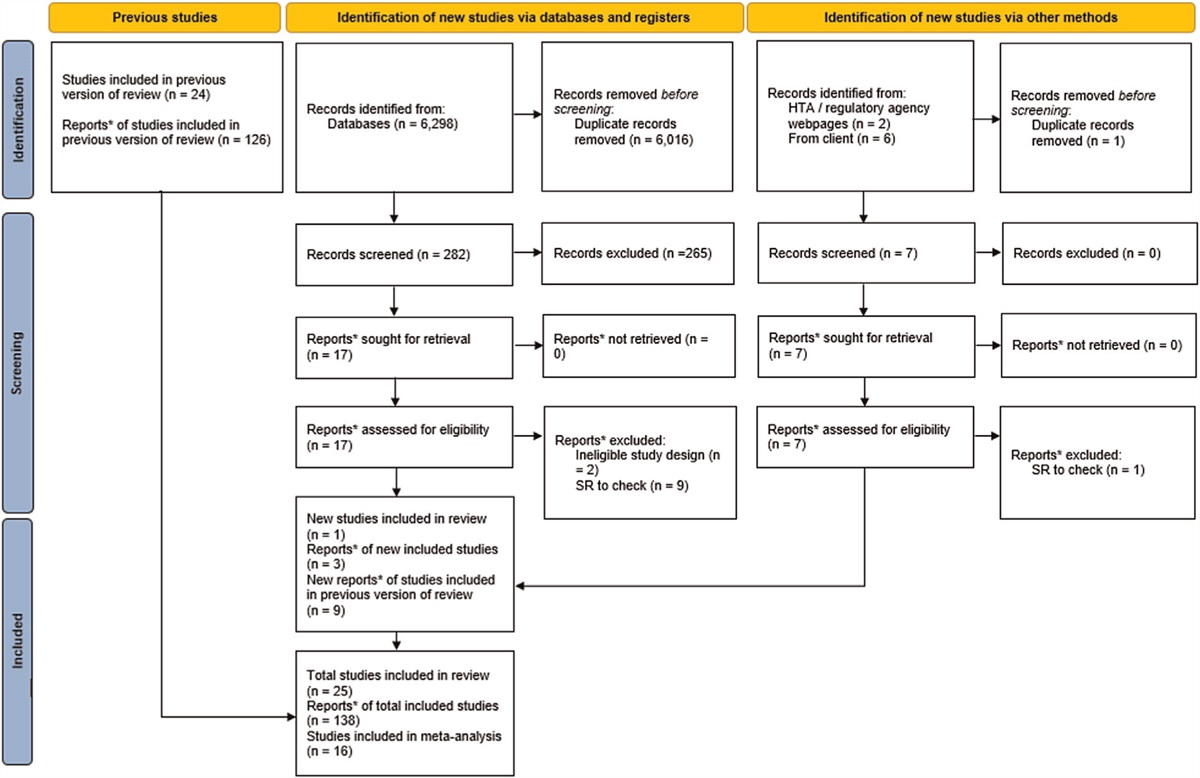
RESULTS Search and screening resultsThe searches were conducted between November and December 2022 and were updated in May 2023. The original searches identified a total of 5905 records, whereby 3980 records remained after deduplication. Twenty-four RCTs (reported in 126 documents) met the eligibility criteria for the systematic review. The updated searches identified an additional 282 records following deduplication. One new RCT was identified as eligible, bringing the total number of included RCTs in the systematic review to 25. Following completion of the searches, an additional publication was identified that provided data for the RADIANCE TRIO trial, which was required for the meta-analysis [31]. Similarly, the results of the SPYRAL HTN-ON-MED trial were published following search completion [16]. The published data [16] were used as the primary reference for SPYRAL HTN-ON-MED in this systematic review and were consistent with the clinical study report initially identified. Figure 1 shows full details of the study selection process as per PRISMA guidelines. The included trials and their associated publications are reported in Supplemental Digital Content 1 Appendix F, https://links.lww.com/HJH/C452.
 FIGURE 1:
FIGURE 1: PRISMA flow diagram of the record selection process.
Risk of bias assessmentNine of the included RCTs were judged to have an overall low risk of methodological bias [15,16,32–38], nine were judged to have ‘some concerns’ [39–47], and seven were judged to have a high risk of methodological bias according the Cochrane Risk of Bias tool [48–54]. A summary of the Risk of Bias Assessment is reported in Supplemental Digital Content 1 Appendix G, https://links.lww.com/HJH/C452.
Conclusion of the feasibility assessment for meta-analysisAll 25 RCTs were considered in the feasibility assessment. One RCT (ISAR-denerve) was excluded from the meta-analysis because the patients had previously received a renal transplant [40]. A further RCT was excluded because it did not report sufficient data to inform the meta-analysis [36].
The feasibility assessment identified that a key difference across the RCTs was the concomitant use of antihypertensive medication with RDN. As such, the RCTs could be categorized into two groups of interest for the meta-analysis:
1. ‘Off-med’ trials: this group included RCTs where RDN was compared with a sham control arm, whereby patients received a renal angiogram but did not receive RDN. In these trials, patients were not permitted to receive antihypertensive medication until at least completion of the primary endpoint. Four RCTs were included in this ‘off-med’ group [15,35,38,49]. 2. ‘On-med’ trials: this group included RCTs where patients who received RDN plus antihypertensive medication were compared with patients who received antihypertensive medication only (in some trials, patients also received sham in the control arm). The regimen in each arm of the trial was the same. Twelve RCTs met the criteria to be included in this ‘on-med’ group [16,32–34,37,42,44–48,51].There were five RCTs that partially met the criteria for the ‘on-med’ group for the meta-analysis [39,41,50,52,53]. However, patients in these RCTs received different medication regimens in each arm. It was, therefore, not possible to isolate and interpret the effect of RDN. These RCTs were excluded from subsequent meta-analyses. A further two RCTs did not meet the criteria to be included in either group as they compared different types of RDN [43,54].
Following consideration of the key differences noted during the feasibility assessment, each outcome was assessed for three groups of trials: the combined on-med and off-med trials, the off-med trials only, and the on-med trials only. Table 1 summarizes the trial characteristics for the off-med and on-med trials. A summary of trial and patient characteristics of all included RCTs is reported in Supplemental Digital Content 1 Appendix H, https://links.lww.com/HJH/C452.
TABLE 1 - Summary of trial characteristics included in the meta-analysis Trial ID Location Primary efficacy outcome measures Duration of follow-up Intervention and comparator Number at baseline Age (years), mean (SD) Gender number (%) male BMI (kg/m2), mean (SD) Office BP at baseline (mmHg), mean (SD) Ambulatory 24 h BP at baseline (mmHg), mean (SD) Ambulatory daytime BP at baseline (mmHg), mean (SD) Off-med trials (n = 4) REDUCE HTN: REINFORCE 12 centres, United States Mean reduction in average 24 h ambulatory SBP at 8 weeks 36 months Vessix RDN system 34 58.5 (10.1) 18a (53a) NR Systolic: 166.3 (9.0)Diastolic: 94.9 (11.8)
Systolic: 148.3 (10.9)Data for TR subgroup (pts with 3 or more meds)
25 centres in the USA, Germany, Japan, UK, Australia, Austria, and Greece Ambulatory BP measurements assessed at 6 months 36 months Symplicity Spyral RDN system + standard antihypertensive medication (either one, two or three drugs) 206 55.2 (9.0) 167a (81.1) 31.4 (6.0) Systolic: 163.0 (7.7)Systolic: 164.8 (7.8) a
Systolic: 149.6 (7.0)Systolic: 151.2 (7.6)
Systolic: 155 (8)Systolic: 162 (7.1)
Systolic: 149.3 (7.0)Systolic: 148.6 (6.2)
Systolic: 154 (8)aBaseline BP for treatment resistant subgroup in SPYRAL HTN-ON MED.
Sixteen RCTs (4 off-med and 12 on-med) were included in the meta-analyses. Office SBP, 24 h ambulatory SBP and ambulatory daytime SBP were the primary outcomes reported across the 16 included studies. These outcomes were prioritized for analysis. Meta-analyses were conducted at primary follow-up and at last follow-up but, because of known confounding factors such as unblinding and differential drug administration across treatment arms at last follow-up, results at last follow-up are reported in Supplemental Digital Content 2, https://links.lww.com/HJH/C453. No significant differences were identified between the on-med and off-med subgroups across most outcomes so, in this section, we focus on the results of the combined analyses. This section reports the results of the random effects model, which was considered to be the most appropriate model because of the clinical heterogeneity identified across the trials [55]. Full results of both the fixed and random effects meta-analysis of all outcomes assessed, and the subgroup and sensitivity analyses conducted at primary follow-up, are presented in Supplemental Digital Content 2, https://links.lww.com/HJH/C453.
Office SBP: overall meta-analysis results and subgroup analysesChange in office SBP at primary follow-up was available for 13 trials (3 off-med and 10 on-med). The random effects meta-analysis suggests that patients randomized to RDN experienced a significantly larger reduction in office SBP compared with patients that did not receive RDN [mean difference between arms (MD) − 8.5 mmHg (95% CI −13.5 to −3.6, I2 75%)) (Fig. 2 a). The SYMPLICITY HTN-2 trial was identified as an outlier that substantially contributed to the overall heterogeneity for all office BP outcomes. When removed, heterogeneity was reduced and results were still significantly in favour of RDN at primary follow-up [mean difference: −5.6 mmHg (95% CI: −7.2 to −4.0, I2 0%)]. Results were consistently in favour of RDN for the treatment-resistant subgroup (sensitivity analysis removing the outlier HTN-2, mean difference: −4.8 (95% CI: −7.8 to −1.8, I2 19%) and all other subgroups and sensitivity analyses explored. Full meta-analysis results for office SBP are shown in Table 2.
 FIGURE 2:
FIGURE 2: Forest plots of renal denervation versus control for blood pressure outcomes. The meta-analysis of the following BP outcomes at primary follow-up: (a) office SBP (b) 24-h ambulatory SBP (c) and daytime ambulatory SBP. BP, blood pressure.
 FIGURE 2 (Continued):
FIGURE 2 (Continued): Forest plots of renal denervation versus control for blood pressure outcomes. The meta-analysis of the following BP outcomes at primary follow-up: (a) office SBP (b) 24-h ambulatory SBP (c) and daytime ambulatory SBP. BP, blood pressure.
TABLE 2 - Meta-analysis results showing the difference
Comments (0)