Clinical practice guidelines recommend measuring blood pressure (BP) outside of the office setting to confirm the diagnosis of hypertension among people with high office BP and to rule out the presence of masked hypertension among individuals without high office BP [1,2]. Ambulatory BP monitoring (ABPM) has been used to measure BP outside of the office setting for several decades [3,4]. Typically, ABPM involves wearing a BP cuff for 24 h with SBP and DBP being measured every 15–30 min [5]. Most ABPM devices come with software that provides estimates of the mean SBP and DBP while individuals are awake, asleep, and over the full 24 h monitoring period. Higher mean awake, asleep, and 24 h SBP are each associated with increased risk for cardiovascular disease (CVD) independent of SBP measured in the office setting [6,7]. In some studies, asleep SBP has demonstrated a stronger association with cardiovascular events when compared with awake and 24 h SBP [7,8].
Using plethysmographic tracings, a diurnal BP pattern in humans was identified in the late 1890s with lower SBP and DBP during sleep versus while awake [9]. By the 1980s, there were extensive data from intra-arterial measurements and ABPM confirming this diurnal BP pattern [10]. In 1988, O’Brien et al. reported that the prevalence of stroke was higher in a group of patients with SBP or DBP that did not decline by at least 10 or 5 mmHg, respectively, from daytime to nighttime (8.00 a.m.–12.00 a.m. to 12a.m.–8 a.m.) [11]. Several subsequent studies have reported higher risk for CVD among adults who do not experience a greater than 10% decline in SBP, and sometimes DBP, from being awake to asleep, a phenotype called nondipping BP [6,7]. Along with mean awake, asleep, and 24 h SBP and DBP mentioned above, the software provided with most ABPM devices also report the percentage decline in SBP and DBP from being awake to asleep. Using this information, nondipping SBP and DBP can be identified easily.
Higher mean nighttime BP has been reported among people with nondipping versus dipping BP [12]. This has led to speculation that the higher CVD and mortality risk associated with nondipping BP may be due to high nighttime BP. Evaluating the association of BP dipping with all-cause and CVD mortality is the focus of the study by de la Sierra and colleagues published in the current issue of the Journal of Hypertension. Following up on a prior analysis reporting the strong associations of nighttime BP with all-cause and cardiovascular mortality [8], the investigators evaluated the association between the daytime-to-nighttime decline in BP and these outcomes. In addition, they assessed the association of all-cause and cardiovascular mortality with abnormal versus normal SBP dipping cross-categorized with abnormal versus normal nighttime SBP. For this analysis, the investigators defined normal dipping SBP (i.e. dipping SBP) as day–night decline in SBP greater than 10%, abnormal dipping SBP (i.e. nondipping SBP) as a day–night decline in SBP 10% or less, and normal (i.e. not high) and abnormal (i.e. high) mean nighttime SBP as less than 120 mmHg and at least 120 mmHg, respectively. The investigators analyzed data from the Spanish ABPM Registry, which included 59 124 adult patients who completed ABPM between 2004 and 2014. All-cause and cardiovascular mortality were assessed over a median follow-up period of almost 10 years. In this study, each 8.2% smaller decline in daytime-to-nighttime SBP and 9.1% smaller decline in daytime-to-nighttime DBP (i.e. representing a standard deviation) was associated with covariate-adjusted hazard ratios of 1.15 and 1.16 for all-cause mortality, respectively, and 1.17 and 1.19 for cardiovascular mortality, respectively. In addition, compared with patients with normal SBP dipping and normal nighttime SBP, the hazard ratio for cardiovascular mortality was 1.17 for patients with abnormal SBP dipping and normal nighttime SBP, 1.62 for patients with normal SBP dipping and abnormal nighttime SBP, and 1.90 for patients with abnormal SBP dipping and abnormal nighttime SBP. From this analysis, the hazard ratio for abnormal versus normal SBP dipping was 1.17 among those with abnormal nighttime SBP (i.e. estimated by 1.90 divided by 1.62), the same as among those with normal nighttime SBP. Also, compared with those with normal SBP dipping and normal nighttime SBP, the hazard ratio for all-cause mortality was 1.13 for patients with abnormal SBP dipping and normal nighttime SBP, 1.38 for patients with normal SBP dipping and abnormal nighttime SBP, and 1.56 for patients with abnormal SBP dipping and abnormal nighttime SBP. The association with all-cause mortality for abnormal versus normal SBP dipping for those with abnormal nighttime SBP was 1.13 (i.e. estimated by 1.56 divided by 1.38), again the same as for those with normal nighttime SBP. Based on these results, the authors concluded that nondipping SBP was associated with increased risk for all-cause and cardiovascular mortality among those with normal nighttime SBP and that nondipping SBP and high nighttime SBP have additive effects on mortality.
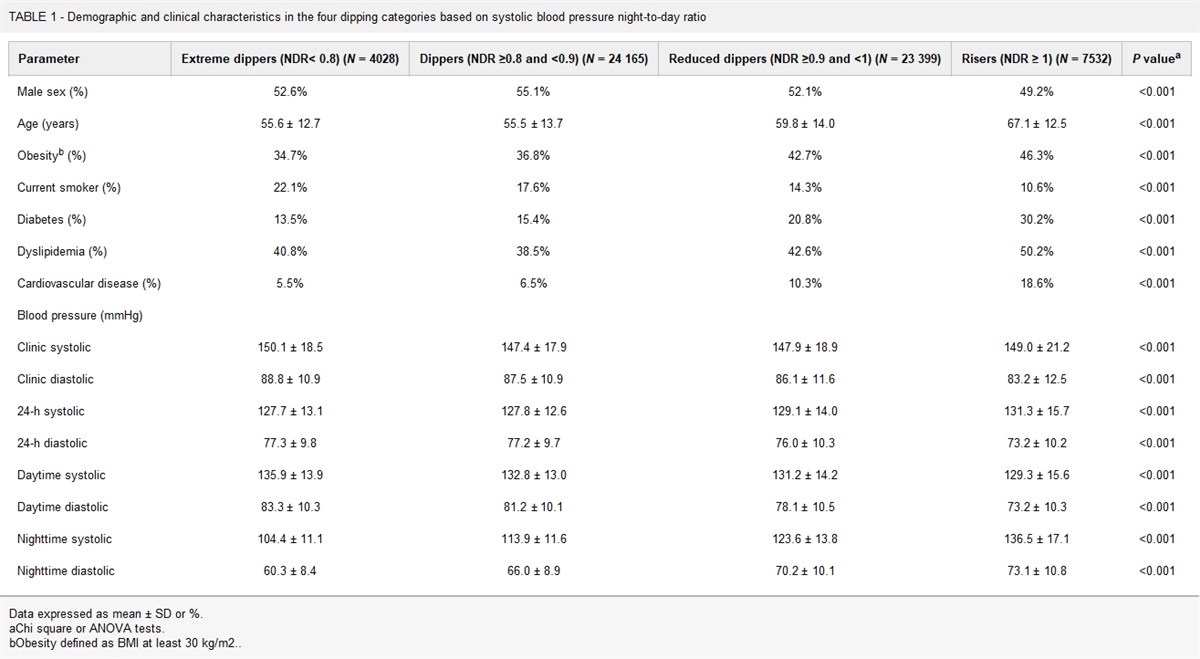
The investigators should be congratulated for studying an important topic using a well established database. The large sample size, and long-term follow-up for all-cause and cardiovascular mortality are major strengths of the Spanish ABPM Registry. However, the results of this study may be open to an alternative conclusion. As stated by the authors, the association of cardiovascular mortality with abnormal versus normal nighttime SBP was substantially stronger [i.e. hazard ratio for cardiovascular mortality of 1.62 for those with normal SBP dipping and for those with abnormal SBP dipping (1.90/1.17 = 1.62)] than with abnormal versus normal SBP dipping [i.e. hazard ratio for cardiovascular mortality of 1.17 for those with normal nighttime SBP and those with abnormal nighttime SBP (1.90/1.62 = 1.17)]. Given the modest hazard ratios for abnormal SBP dipping, we wondered whether residual confounding might be present. Residual confounding can occur in observational studies when a statistical analysis does not adequately control for confounding [13]. By treating nighttime SBP as a binary measure (abnormal versus normal), the study could have under-controlled or over-controlled for nighttime SBP if there are differences in nighttime SBP for those with abnormal versus normal SBP dipping within either the normal or abnormal nighttime SBP category. As shown in Table 5 of their article, the mean nighttime SBP was 4.0 mmHg higher (111.5 versus 107.5 mmHg) among those with abnormal versus normal SBP dipping in the normal nighttime SBP stratum and 6.8 mmHg higher (135.2 versus 128.4 mmHg) in the abnormal nighttime SBP stratum. These data demonstrate that the abnormal dipping and normal dipping categories were not matched in terms of nighttime SBP for either those with normal or those with abnormal nighttime SBP.
In a prior study using Spanish ABPM Registry data, each 11.5 mmHg higher nighttime SBP was associated with hazard ratios for all-cause and cardiovascular mortality of 1.40 and 1.46, respectively [8]. Accordingly, 4.0 and 6.8 mmHg higher nighttime SBP would be associated with hazard ratios of 1.12 and 1.22 for all-cause mortality, respectively, and 1.14 and 1.25 for cardiovascular mortality, respectively. Based on these calculations, the higher nighttime SBP among those with abnormal versus normal SBP dipping can explain nearly all of the excess risk for all-cause and cardiovascular mortality reported for abnormal SBP dipping among those without high nighttime SBP and all of the excess risk reported for abnormal SBP dipping among those with high nighttime SBP.
Overall, the Spanish ABPM Registry data raise doubt about the prognostic value of nondipping SBP as a risk factor for all-cause and CVD mortality. In addition, prior studies have reported low reproducibility for day–night BP ratios. Using data from a published study in which 414 adults not taking antihypertensive medication completed two 24 h ABPM periods within a 4-week period, we calculated the kappa statistic for nondipping SBP to be 0.45 [14]. In our Improving the Detection of Hypertension study (N = 364 adults not taking antihypertensive medication, also with two 24 h ABPM recordings completed 3–4 weeks apart), the kappa statistic for nondipping SBP is 0.36, substantially lower than for mean awake SBP at least 130 mmHg (kappa = 0.71) and mean asleep SBP at least 110 mmHg (kappa = 0.67) [15]. These data show that nondipping SBP has relatively poor reproducibility, further limiting its utility for CVD risk prediction.
In conclusion, the study by de la Sierra and colleagues provides important data on nighttime BP, BP dipping, and all-cause and cardiovascular mortality risk. The associations of abnormal SBP dipping with all-cause and cardiovascular mortality were weak and we have shown that these associations may be explained by the higher nighttime SBP of those with abnormal dipping. Based on these data along with prior studies that have demonstrated the low reproducibility of the nondipping BP phenotype, we think SBP and DBP dipping may not be useful for clinical decision-making. Perhaps, software-generated ABPM reports should not even provide BP dipping but just present mean awake, asleep, and 24 h SBP and DBP.
ACKNOWLEDGEMENTS
Conflicts of interest
There are no conflicts of interest.
REFERENCES
1. Whelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, Dennison Himmelfarb C, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2018; 71:1269–1324.
2. Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J 2018; 39:3021–3104.
3. Kain HK, Hinman AT, Sokolow M. Arterial blood pressure measurements with a portable recorder in hypertensive patients. I. Variability and correlation with ‘casual’ pressures. Circulation 1964; 30:882–892.
4. Pickering TG, Gerin W, Schwartz AR. What is the white-coat effect and how should it be measured? Blood Press Monit 2002; 7:293–300.
5. Pickering TG, Shimbo D, Haas D. Ambulatory blood-pressure monitoring. N Engl J Med 2006; 354:2368–2374.
6. Yano Y, Tanner RM, Sakhuja S, Jaeger BC, Booth JN 3rd, Abdalla M, et al. Association of daytime and nighttime blood pressure with cardiovascular disease events among African American individuals. JAMA Cardiol 2019; 4:910–917.
7. Yang WY, Melgarejo JD, Thijs L, Zhang ZY, Boggia J, Wei FF, et al. International Database on Ambulatory Blood Pressure in Relation to Cardiovascular Outcomes (IDACO) Investigators. Association of office and ambulatory blood pressure with mortality and cardiovascular outcomes. JAMA 2019; 322:409–420.
8. Staplin N, de la Sierra A, Ruilope LM, Emberson JR, Vinyoles E, Gorostidi M, et al. Relationship between clinic and ambulatory blood pressure and mortality: an observational cohort study in 59 124 patients. Lancet 2023; 401:2041–2050.
9. Hill L. On rest, sleep and work and the concomitant changes in the circulation of the blood. The Lancet 1898; 151:282–285.
10. Millar-Craig MW, Bishop CN, Raftery EB. Circadian variation of blood-pressure. Lancet 1978; 1:795–797.
11. O’Brien E, Sheridan J, O’Malley K. Dippers and nondippers. Lancet 1988; 2:397.
12. de la Sierra A, Redon J, Banegas JR, Segura J, Parati G, Gorostidi M, et al. Spanish Society of Hypertension Ambulatory Blood Pressure Monitoring Registry Investigators. Prevalence and factors associated with circadian blood pressure patterns in hypertensive patients. Hypertension 2009; 53:466–472.
13. Kyriacou DN, Lewis RJ. Confounding by indication in clinical research. JAMA 2016; 316:1818–1819.
14. Cuspidi C, Meani S, Salerno M, Valerio C, Fusi V, Severgnini B, et al. Reproducibility of nocturnal blood pressure fall in early phases of untreated essential hypertension: a prospective observational study. J Hum Hypertens 2004; 18:503–509.
15. Schwartz JE, Muntner P, Kronish IM, Burg MM, Pickering TG, Bigger JT, et al. Reliability of office, home, and ambulatory blood pressure measurements and correlation with left ventricular mass. J Am Coll Cardiol 2020; 76:2911–2922.






Comments (0)