
Remember me

Between August 2016 and January 2018, consecutive patients who underwent MRI post cystoscopy for bladder cancer at our institution and meeting study eligibility criteria were identified. The local institutional ethics committee approved this retrospective study, with the need to obtain informed consent waived (NRES Committee East of England, UK, reference A093248). The inclusion criteria were (a) biopsy-proven bladder cancer, (b) bladder MRI including T1-weighted images (T1WI), T2-weighted images (T2WI) and DWI within 6 weeks of TURBT performed at our institution and (c) either cystectomy or follow-up cystoscopy within 90 days. 62 patients met the initial inclusion criteria, with 21 patients excluded due to concurrent treatment with intravesical BCG, systemic chemotherapy or radiotherapy (n = 14), absence of muscle in the biopsy specimen (n = 3), poor quality T2WI/DWI owing to motion artefact or hip prosthesis (n = 3), or debris obscuring the bladder wall at cystoscopy (n = 1), giving a final eligible study cohort of 41 patients (Fig. 1).
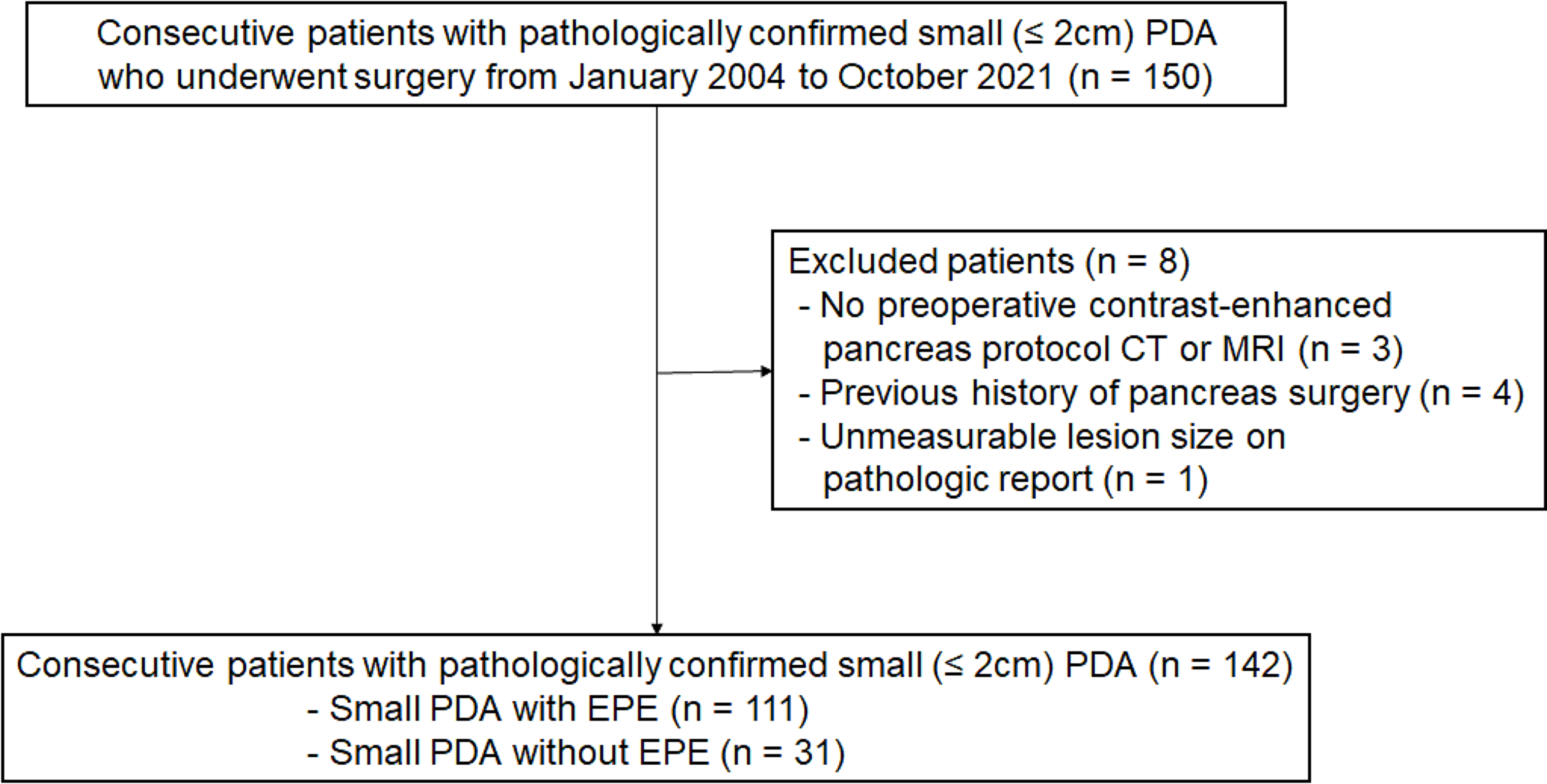
Fig.1
Flow diagram showing patient enrolment
MRI protocolPatients underwent bladder MRI using a 1.5 T MR450 (GE Healthcare, Waukesha, WI, USA) with a 16-channel phased array body coil. Unless contraindicated, intravenous injection of hyoscine butylbromide (Buscopan, 20 mg/ml, Boehringer, Germany) was administered prior to imaging to reduce peristaltic movement. Conventional T1-weighted spin-echo images (449 ms repetition time (TR), 9 ms echo time (TE); 352 × 224 matrix; 24 × 24 cm field-of-view (FOV); 5 mm slice thickness; 2.5 mm intersection gap; one signal acquired) in the axial plane. High-resolution T2 weighted turbo spin-echo images (3700 ms TR, 86 ms TE; 320 × 288 matrix; 24 × 24 cm field-of-view (FOV); 3 mm slice thickness; 1 mm intersection gap; two signals were acquired. Images were obtained in three orthogonal planes. Diffusion-weighted imaging (DWI) was performed using a spin-echo echo-planar imaging pulse sequence (5000 ms TR, 78 ms TE; 128 × 128 matrix; 27 × 27 cm field-of-view (FOV); 4.5 mm slice thickness; 0 mm intersection gap with b-values of 0 and 1000 s/mm2. Apparent diffusion coefficient (ADC) maps were calculated automatically.
Image analysisMR images were retrospectively evaluated by two subspecialist uroradiologists with 12 years (TB) and 6 years (NS) of experience in reading bladder MRI. Both readers reviewed MRI studies independently and were blinded to clinical data and pathology reports. Each reader independently assessed T1WI and T2WI together and T1WI, T2WI and DWI combined and assigned the perceived likelihood of tumour using a Likert scale: 1 = definitely absent, 2 = possibly absent, 3 = indeterminate, 4 = possibly present and 5 = definitely present. For each lesion size, location and T-categorisation was evaluated using the 8th edition of the American Joint Committee on Cancer (AJCC) staging manual [18]. In brief, readers assessed T1WI to look for haematoma, T2WI to look for a continuous low signal intensity line in the bladder wall that represents an intact muscularis propria and DWI (high b-value images) for tumour which is hyperintense with corresponding hypointensity on ADC maps. To minimise learning bias the second reading session was performed after a wash-out interval of 4 weeks. Readers only had access to specific sequences when reviewing each set of images. Differences in opinion were resolved by consensus, with the most experienced reader’s opinion considered as definitive.
Histopathologic analysisAll biopsies and surgical specimens were analysed and graded according to existing guidelines [19] by an experienced uropathologist and reviewed by a second uropathologist at a multidisciplinary team meeting. Tumour cell type, and T-category were also obtained. In patients with multiple tumours the tumour with the highest pathological T-category was recorded.
Data analysisDemographic characteristics, MRI data and pathologic data were described with summary statistics. Sensitivity, specificity, positive predictive value (PPV), and negative predictive (NPV) value for detection of tumour using the Likert scale were calculated for both readers, using a 2 × 2 contingency table. For the purpose of data analysis, Likert score 3 was considered as positive for tumour as this reflects how this group of patients would be managed in clinical practice. Accuracy of MRI for T-categorisation was determined for for NMIBC detectable at MRI (< pT2, excluding pTis) and MIBC (≥ pT2). Data was analysed with the statistical package MedCalc (Version 20.305). The receiver operating characteristic (ROC) analysis was performed. Inter-reader agreement was analysed by means of weighted κ values with quadratic weighting (κ = 0.00–0.20, poor; 0.21–0.40, fair; 0.41–0.60, moderate; 0.61–0.80, good; and 0.81–1.00, excellent agreement).
Comments (0)