
Remember me





Aortic stiffness, an important pathophysiologic aspect of large-artery damage, is a predictor of all-cause and cardiovascular mortality [1–3]. Direct quantification of aortic stiffness can be performed noninvasively by measurement of carotid–femoral pulse wave velocity (c-f PWV), which is considered the gold-standard method [1]. Aortic stiffness increases with ageing, diabetes mellitus, chronic kidney diseases, including end-stage renal disease, and other high-risk conditions for cardiovascular diseases [2].
Advanced glycation end products (AGEs) are potentially toxic proteins that become glycated after contact with sugars [3], and are established risk marker in diabetic vascular disease, and associated with the degree of diabetes complications, renal failure, and atherosclerosis [4,5]. By formation of crosslinking and modification of extracellular matrix proteins, AGEs modulate the mechanical properties of the target tissue, causing reduced elasticity and flexibility, thereby promoting arterial stiffness [6], as a marker of early vascular ageing (EVA).
AGEs can be produced endogenously by the influence of oxidative stress or hyperglycaemia; but they can also be consumed exogenously through food intake [7]. Chronological age, oxidative stress, inflammation, kidney function, nutrition, and diet also influence AGE accumulation [8]. Development of therapeutic agents, which break the established AGE cross-link between proteins such as collagen and elastin have emerged as potential therapeutics, such as alagebrium, which could potentially reverse the pathologic effects of AGE [9,10].
Skin AGEs have been found to predict incident type 2 diabetes, cardiovascular disease, and mortality in a middle-aged general population [11]. However, the association between AGEs and arterial stiffness (vascular ageing) has been assessed only in smaller case–control studies with a large prevalence of comorbidities, for example, in diabetes mellitus [12–15], hypertension [16], renal failure [17–20], and in older individuals of the general population [21–24]. In this study, we aimed to evaluate the association between skin AGEs and aortic stiffness in the general population of young to middle-aged adults.
MATERIALS AND METHODS Study population and designThe Malmö Offspring Study (MOS) is a prospective, population-based cohort in Malmö, Sweden, launched in 2013 and completed in 2021 [25]. The cohort consists of 5259 individuals who are children and grandchildren to the index participants in the well established prospective Malmö Diet and Cancer Study, launched in the 90s with over 20 years of follow-up [26]. To ensure that participants in the different generations were directly related, a national taxation authority register in Sweden (NAVET) was used [27]. In total, 2518 individuals had complete data on skin autofluorescence and aortic stiffness and were included in the current study.
Ethical approvalThe MOS study was approved by the Regional Ethics Committee at Lund University (Dnr. 2012/594). The study complies with the Declaration of Helsinki. All participants provided written informed consent.
Assessment of aortic stiffness and vascular ageingDirect, noninvasive assessment of aortic stiffness was performed by the gold-standard method, c-f PWV after 5 min of supine rest using Sphygmocor (AtCor, Australia) [28]. In brief, the distance from the carotid-to-femoral artery was measured directly between each artery and the suprasternal notch. PWV was calculated by measuring the time delay between two characteristic timepoints on two pressure waveforms at a known distance apart. The SphygmoCor method uses the foot of the waveform as an onset point for calculating the time differences between the R wave of the electrocardiogram and the pulse waveforms at each site. PWV was automatically generated as the carotid–femoral artery distance divided by the wave traveling time between the above two sites. Adapted to the expert consensus document by European Society of Hypertension, the standard distance was calculated by using 80% of the direct carotid–femoral (common carotid artery – common femoral artery × 0.8) tape measure distance, as it is the most accurate body surface distance estimate, and less influenced by larger abdomens and breasts [1].
In addition, aortic augmentation index (AIx), an indirect measurement of aortic stiffness, was measured by radial applanation tonometry using PWA Sphygmocor (AtCor, Australia). AIx was standardized to a heart rate of 75 beats per minute (AIx@75) by adjusting the AIx by −4.8 for each 10 bpm above and +4.8 for each 10 bpm below a resting heart rate of 75 bpm.
Measurement of advanced glycation end-productsAdvanced glycation end-products were measured by a well validated, noninvasive method, using skin autofluorescence of AGE with AGE-Reader (DiagnOptics, Groningen, the Netherlands) [29–31]. In brief, skin autofluorescence was measured within a 4 cm2 area on the forearm and defined as the ratio between the emission intensity in the wavelength range between 420 and 600 nm and the reflected excitation intensity with a wavelength between 300 and 420 nm, multiplied by 100, and is expressed in arbitrary units. Skin autofluorescence was adjusted for skin reflectance by the AGE-Reader, by comparisons with spectra from a white standard and from dark measurements. Autofluorescence was calculated by automated off-line analysis. The mean of three values was recorded and used in the analysis [5].
Definition of variables and clinical characteristicsData on prevalent diseases at baseline were collected from The Swedish National Patient Register. Data on treatment with antihypertensives or antidiabetic drugs was acquired from the Swedish National Prescribed Drug Register using ATC-codes of prescribed drugs. Estimated glomerular filtration rate (eGFR) was calculated using the CKD-EPI Creatinine Equation [32]. Current smoking (defined as regular or occasional smoking) was self-reported in the questionnaire. Weight (kg) and height (m) were measured in light indoor clothing, and BMI (kg/m2) was subsequently calculated. Resting blood pressure (mmHg) and heart rate (beats/min) were measured as a mean of two readings in the supine position after 5 min rest by use of an automatic device (Omron M5–1 IntelliSense, the Netherlands). Blood samples were acquired after an overnight fast and stored at −80 °C. Fasting blood samples were analysed for total cholesterol, low-density lipoprotein cholesterol (LDL) and fasting plasma glucose (FPG) at the Department of Clinical Chemistry, Skåne University Hospital in Malmö, participating in a national standardization and quality control system.
Statistical analysesContinuous variables were compared using Student's t tests. Categorical variables were compared using the χ2 test. Variables are presented as means ± standard deviation (SD), whereas categorical variables are displayed as frequencies. We stratified subjects by age into two groups 50 years or less and older than 50 years. This cut-off was specified a priori considering that changes in AIx are more prominent in individuals below 50 years, whereas changes in carotid–femoral PWV are more marked in those older than 50 years [33–35]. AGEs were assessed by quartiles using one-way analysis of variance (ANOVA). Linear regression was performed to analyse the association between PWV, AIx@75 (dependent variable) and AGEs (independent variable) in a univariate model and adjusted model for traditional cardiovascular risk factors such as: sex, BMI, SBP, heart rate, fasting plasma glucose, estimated glomerular filtration rate (eGFR), LDL cholesterol, prevalent diabetes, and current smoking. To determine the specific sensitivity and specificity values of AGEs in relation to PWV and AIX@75, unadjusted ROC curve analysis was performed. A P value of less than 0.05 was considered statistically significant. All statistical analyses were performed in IBM SPSS Statistics 28 (IBM Corporation, Armonk, New York, USA).
RESULTS Study characteristicsThe study characteristics are displayed in Table 1. The mean age of participants in the younger group was 33.3 ± 9.7 years compared with the older group 57.3 ± 4.4 years (P < 0.001). The distribution of women was equal in both groups, around 52%. The overall prevalence of comorbidities was low in the general population, approximately 4% had prevalent diabetes mellitus or hypertension.
TABLE 1 - Study characteristics of the population General population (n = 2518) Subjects ≤50 years old (n = 1689) Subjects >50 years old (n = 829) P-value Age (years ± SD) 41.8 ± 14.5 33.3 ± 9.7 57.3 ± 4.4 <0.001 Sex, women (%) 52.2 52.2 52.7 0.80 BMI (kg/m2 ± SD) 25.9 ± 4.7 25.3 ± 4.7 26.9 ± 4.5 0.72 Current smoking (%) 12.9 14.4 10.1 0.003 Fasting glucose (mmol/l ± SD) 5.5 ± 1.1 5.3 ± 0.9 5.7 ± 1.3 <0.001 HbA1c (mmol/mol ± SD) 34.8 ± 6.6 33.3 ± 5.4 37.2 ± 7.3 <0.001 LDL (mmol/l ± SD) 3.2 ± 1.0 2.9 ± 0.9 3.5 ± 1.0 <0.001 Triglyceride/HDL ratio (mg/dl ± SD) 1.9 ± 1.8 1.8 ± 1.7 2.1 ± 1.9 <0.001 eGFR mean (ml/min/1.73 m2) 93.8 ± 16.1 98.9 ± 15.2 83.7 ± 12.7 <0.001 eGFR <60 ml/min/1.73 m2 (%) 1.2 0.2 1.0 0.29 SBP (mmHg ± SD) 116.8 ± 15.1 112.3 ± 12.1 125.9 ± 16.4 <0.001 HR (bpm ± SD) 62.8 ± 10.1 63.6 ± 10.5 61.1 ± 9.4 <0.001 Advanced glycation end products (AU ± SD) 1.7 ± 0.5 1.6 ± 0.3 2.1 ± 0.4 0.03 Treatment (%) Antihypertensive 7.2 2.6 17.1 <0.001 Antidiabetic 1.7 1.0 4.8 <0.001 Prevalent disease (%) Atrial fibrillation 0.7 0.4 1.4 0.004 Diabetes mellitus 3.8 2.1 7.1 <0.001 Hypertension 4.0 1.0 10.4 <0.001 Stroke 0.8 0.2 1.9 <0.001 Aortic stiffness measurements c-f PWV (m/s ± SD) 7.4 ± 1.5 6.8 ± 1.1 8.6 ± 1.6 <0.001 Aix@75 (mean % ± SD) 8.0 ± 14.6 2.0 ± 12.7 20.4 ± 10.2 <0.001Aix@75 augmentation index calibrated for a standard heart rate of 75 bpm; AU, arbitrary units; BP, blood pressure; c–f, carotid–femoral; eGFR, estimated glomerular filtration rate; HbA1c, hemoglobin A1c; HDL, high-density lipoprotein; HR heart rate; LDL, low-density lipoprotein; PWV, pulse wave velocity; SD, standard deviation.
The mean level of skin AGEs was 1.7 AU in the general population and differed significantly between both age groups, with lower levels observed in younger individuals (1.6 ± 0.3 versus 2.1 ± 0.4 AU, P = 0.03). Equally, as expected, measures of direct (PWV P < 0.001) and indirect (AIX@75 P < 0.001) aortic stiffness were significantly higher in the older group.
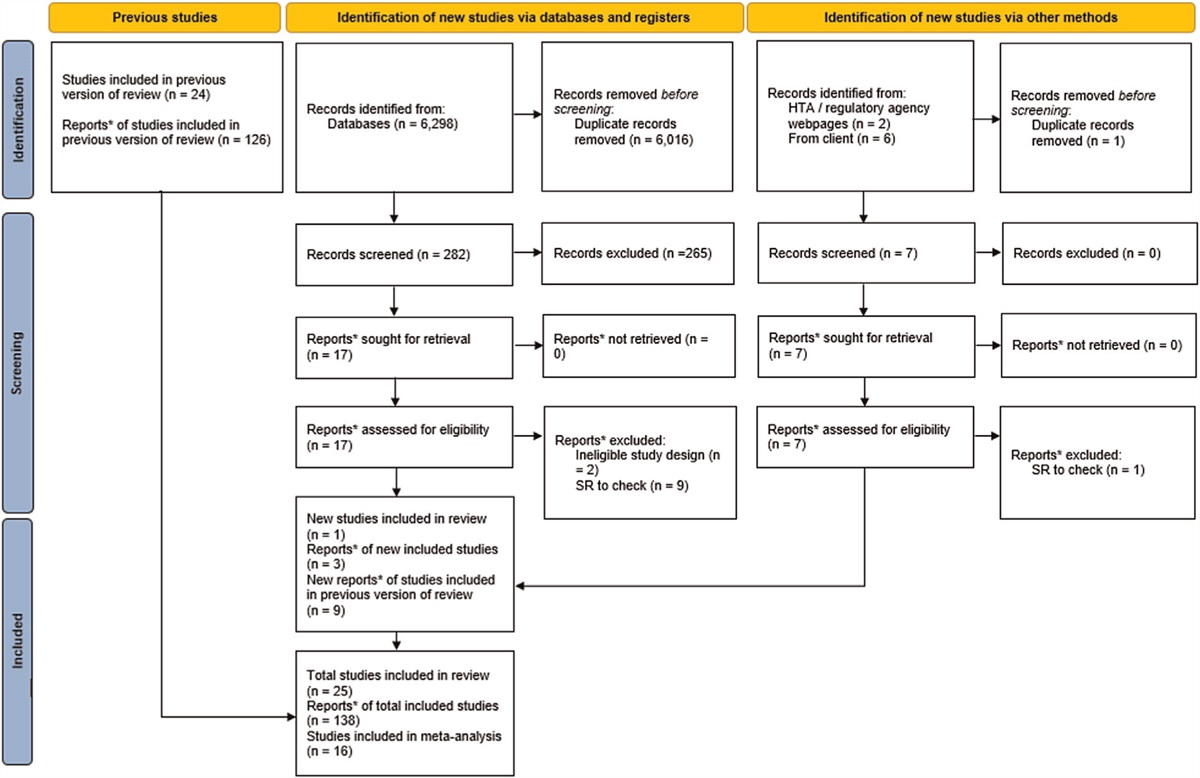
Association between skin advanced glycation end products and vascular ageing in the general population and stratified by 50 years of ageThe distribution of AGE across all four quartiles demonstrated an overall linear relationship with measurements of PWV and AIX@75 (vascular ageing) with a gradual increase in aortic stiffness with higher levels of AGEs (Figs. 1 and 2, Supplementary Figures 1 and 2, https://links.lww.com/HJH/C353 and Table 2). This pattern was most evident among younger individuals.
 FIGURE 1:
FIGURE 1: The distribution of skin advanced glycation end products in relation to measurements of direct (pulse wave velocity) vascular ageing stratified by 50 years of age. (a) Pulse wave velocity in individuals 50 years old or less. (b) Pulse wave velocity in individuals greater than 50 years old. AGEs, advanced glycation end products; PWV, pulse wave velocity; Q, quartile.
 FIGURE 2:
FIGURE 2: The distribution of skin advanced glycation end products in relation to measurements of indirect (augmentation index) vascular ageing stratified by 50 years of age. (a) Augmentation index in individuals 50 years old or less. (b) Augmentation index in individuals greater than 50 years old. AGEs, advanced glycation end products; Aix@75, augmentation index calibrated for a standard heart rate of 75 bpm; Q, quartile.
TABLE 2 - Measurements of aortic stiffness as a marker of vascular ageing, stratified according to quartiles of advanced glycation end products in the general population and stratified by 50 years of age Quartiles of AGEs in the general population Quartiles of AGEs in younger subjects (≤50 years old) Quartiles of AGEs in older subjects (>50 years old) Mean ± SD P value Mean ± SD P value Mean ± SD P value PWV (m/s) Q1 6.48 ± 1.03 P < 0.001 Q1 6.3 ± 0.9 P < 0.001 Q1 8.4 ± 1.3 P = 0.03 Q2 7.18 ± 1.37 Q2 6.6 ± 1.0 Q2 8.4 ± 1.5 Q3 7.75 ± 1.43 Q3 6.9 ± 1.2 Q3 8.6 ± 1.6 Q4 8.26 ± 1.70 Q4 7.3 ± 1.2 Q4 8.8 ± 2.0 AIX@75 (mean %) Q1 −1.59 ± 11.92 P < 0.001 Q1 −3.1 ± 10.7 P < 0.001 Q1 18.5 ± 10.2 P < 0.001 Q2 5.28 ± 13.75 Q2 −0.8 ± 12.5 Q2 18.9 ± 10.4 Q3 11.71 ± 13.20 Q3 3.6 ± 12.4 Q3 21.3 ± 9.5 Q4 17.41 ± 12.14 Q4 7.3 ± 12.3 Q4 23.4 ± 9.6AGEs, advanced glycation end products; Aix@75, augmentation index calibrated for a standard heart rate of 75 bpm; PWV, pulse wave velocity; Q, quartile.
In the univariate linear regression model, higher levels of skin AGEs were associated with increased aortic stiffness assessed by PWV and AIX@75 in both younger and older individuals (P < 0.001, Table 3, model 1). Following adjustment, we found that increased levels of skin AGEs were significantly associated with higher direct aortic stiffness (PWV) in younger individuals 50 years old or less (unstandardized beta coefficient β, 0.55 m/s, P < 0.001, Table 3, model 2); however, not in older individuals (β 0.23 m/s, P = 0.10). On the other hand, indirect aortic stiffness as assessed by mean AIx@75, was significantly associated with higher levels of skin AGEs in both younger individuals (β 7.78, P < 0.001) and older individuals (β 3.69, P < 0.001) in the adjusted linear regression model.
TABLE 3 - Linear regression analysis assessing the association between advanced glycation end products and vascular ageing in the general population (n = 2518) and stratified by 50 years of age General population (n = 2518) Subjects ≤50 years old (n = 1689) Subjects >50 years old (n = 829) Model 1 PWV (m/s) β 1.55Linear regression analysis with reported unstandardized beta-coefficient (β). PWV and AIX@75 entered as dependent variable. AGEs entered as independent variable. Model 1: unadjusted model. Model 2: adjusted for sex, BMI, SBP, heart rate, fasting plasma glucose, estimated glomerular filtration rate, low-density-lipoprotein cholesterol, prevalent diabetes, current smoking, as well as age in model 2 of the general population. AGEs, advanced glycation end products; Aix@75, augmentation index calibrated for a standard heart rate of 75 bpm; PWV, pulse wave velocity.
Using ROC analysis, the optimal cut-off value of skin AGEs to predict vascular ageing for individuals in the highest quartile of PWV of the general population was 1.85 AU, generating an area under the curve (AUC) of 0.74 (sensitivity of 62% and 1-specificity of 26%, Supplementary Figure 3A, https://links.lww.com/HJH/C353). Correspondingly, the optimal cut-off value of skin AGEs for individuals in the highest quartile of AIX@75 in the general population was 1.75 AU, generating an AUC of 0.75 (sensitivity of 74% and 1-specificity of 36%, Supplementary Figure 3B, https://links.lww.com/HJH/C353).
DISCUSSIONIn this population-based study of young and middle-aged adults, we observed higher levels of skin AGEs in younger individuals with increased aortic stiffness (higher PWV), as a marker of vascular ageing, independent of cardiometabolic risk factors and prevalent diabetes compared with older adults. On the contrary, an indirect measure of vascular ageing (higher AIx) was increased in both age groups.
To date, the association between AGEs and arterial stiffness (vascular ageing) has been assessed in subjects with diabetes mellitus or chronic kidney disease [13–15,17–19], as well as in the general population with a higher prevalence of comorbidities [12,22,23]. However, we present here the largest population-based study to date comprising of younger adults (mean age 41 years) [14]. Moreover, in addition to assessment of direct aortic stiffness using c-f PWV, we also assessed an indirect measure of aortic stiffness, AIx. Our findings are in line with previous studies who have investigated the association between AGEs and arterial stiffness across older individuals and in different patient groups [21–24]. The results support the notion that higher levels of AGEs contribute to increased vascular ageing, independent of traditional cardiometabolic risk factors.
In a systematic review and meta-analysis comprising mostly patients with diabetes and chronic kidney disease, a positive weak association between increased levels of AGEs and pulse wave velocity, as well as with subclinical atherosclerosis (intima–media thickness), was found [36]. These findings suggest that measurement of AGE by skin autofluorescence can be considered when assessing early stages of cardiovascular risk, although more prospective studies are needed to evaluate the appropriateness of using AGEs for routine assessment in clinical practice.
Another meta-analysis of over 79 000 consisting largely of patients with diabetes and chronic kidney disease assessed prospectively, found that higher levels of skin AGEs were significantly correlated with higher pooled risk of major adverse cardiovascular events (MACE) (pooled hazard ratio: 1.54, 95% CI: 1.31–1.81, I2 = 68%), as well as fatal and nonfatal cardiovascular disease (hazard ratios 1.88 and 1.40, respectively) [37], thus being a good and valuable biomarker for predicting MACE. Similarly, skin AGEs can predict risk of incident diabetes type 2 [11], thus providing clinically valuable information when screening for future risk of diabetes, independent of glycaemic measures and the metabolic syndrome.
Among individuals diagnosed with coronary artery disease, there was a significant correlation between skin autofluorescence, vessel stiffness, and the AGE autofluorescence observed in the collagenase digestible collagen fraction derived from residual bypass graft material, suggesting that the noninvasive skin autofluorescence might reflect vascular modifications in situ[38]. Although the precise mechanisms remain incompletely understood, there is also evidence suggesting that skin autofluorescence mirrors systemic nonenzymatic glycation processes. Our prior research has demonstrated a notable correlation between heightened AGE accumulation, quantified through skin autofluorescence, and discernible declines in lung function, signifying alterations in the lung parenchyma [39].
AGEs play a significant role in contributing to vascular damage through various mechanisms. Nonenzymatic protein glycation involves a complex sequence of reactions, the so-called Maillard reaction, resulting in the formation of early glycation products that eventually transform into AGEs [3]. Reduced renal clearance of AGE precursors can further contribute to the accumulation of these end products [40]. The build-up of chemically stable AGEs from long-lived proteins can serve as an indicator of cumulative metabolic stress [41]. One important way in which AGEs contribute to vascular damage is through the formation of cross-links between collagen fibres of the aortic media. Collagen is a major structural component of blood vessels, providing strength and elasticity. However, when AGEs accumulate, they can induce abnormal cross-linking of collagen fibres, leading to increased arterial stiffness and reduced vascular compliance. This phenomenon results in the loss of arterial elasticity and the consequent impairment of vascular function [6].
Moreover, AGEs can activate receptors for advanced glycation end products (RAGE) present on various cell types within the blood vessel walls. Activation of RAGE triggers intracellular signalling pathways that promote inflammation, oxidative stress, and fibrosis [42]. The activation of RAGE by AGEs leads to the production and release of pro-inflammatory cytokines, chemokines, and adhesion molecules, that attract immune cells to the site of vascular damage, promoting chronic inflammation within the vessel walls [43]. Inflammatory processes can induce endothelial dysfunction [44], disrupt the balance of vasoactive substances, and stimulate the proliferation and migration of smooth muscle cells, all of which contribute to vascular disorder [45]. Furthermore, the AGE–RAGE interaction triggers the generation of reactive oxygen species (ROS) and impairs the antioxidant defence mechanisms of endothelial cells [46,47]. Excessive production of ROS can cause damage to the vascular endothelium [44], initiate lipid peroxidation [48], promote the formation of pro-inflammatory molecules, and contribute to the progression of vascular damage.
Additionally, AGEs can stimulate the production of fibrotic components, such as collagen and fibronectin, in the vessel walls. The increased deposition of these fibrotic components leads to the thickening and remodelling of arterial walls, further impairing vascular function and promoting the development of vascular diseases [49].
In summary, AGEs contribute to vascular damage through the formation of collagen cross-links, activation of RAGE-mediated pathways leading to inflammation and oxidative stress, and the stimulation of fibrotic processes. These mechanisms collectively promote endothelial dysfunction, arterial stiffness, chronic inflammation, oxidative damage, and structural alterations in the blood vessels, ultimately contributing to the development and progression of vascular diseases.
Clinical relevanceOur findings emphasize the importance of considering AGEs as a potential target for interventions aimed at preventing or mitigating vascular ageing, even in younger individuals without significant comorbidities. Early identification and management of AGE-related processes may in turn have implications for maintaining cardiovascular health and preventing the development of age-related vascular diseases. The interventions might include lifestyle changes, including dietary adjustments (limiting sugar intake and incorporating antioxidant-rich foods), regular exercise and abstaining from smoking and excessive alcohol consumption. Additionally, compounds like carnosine and vitamin B6 have shown promise in inhibiting AGE formation [50,51]. Although complete prevention is challenging because of the natural ageing process, a combination of these measures, along with a balanced diet, could be expected to contribute to lowering of AGE accumulation.
Study strengths and limitationsOur study has both strengths and limitations. Through the utilization of a sizably extensive cohort that was thoroughly characterized, we effectively secured sufficient statistical power to support the validity and robustness of our research findings. We implemented diligent adjustments to mitigate the potential influence of established clinical confounding factors. However, the present study also has certain limitations. Firstly, it is a single-centre study, which restricts the generalizability of our findings to broader populations. Additionally, the cross-sectional design of the study prevents the conclusions of causal relationships.
In conclusion, our findings show that higher levels of advanced glycation end products are positively associated with increased direct and indirect vascular ageing in younger individuals, independent of cardiometabolic risk factors. Future studies are warranted to elucidate the effect of reduced dietary intake of AGE and AGE-inhibition on aortic stiffness in the general population.
ACKNOWLEDGEMENTSConcept and design: M.J. Acquisition of data: P.M.N. Statistical analysis: M.J. Interpretation of data: M.J., A.J., G.E., P.M.N. Drafting of the manuscript: M.J., A.J. Critical revision and approval of the manuscript M.J., A.J., G.E., P.M.N. We acknowledge support from the Lund University Infrastructure grant to the ”Malmö population-based cohorts” (LU STYR 2019/2046). We thank data manager Anders Dahlin for his extensive and exceptional work with quality control of MOS data, and the staff at the Clinical Research Unit, Department of Internal Medicine, SUS, Malmö, for their dedicated work.
Sources of funding: this study was funded by the Research Council of Sweden (Grant 521-2013-2756), the Swedish Heart and Lung Foundation (grants 2015-0427 and 2021-0348), Swedish governmental funding of clinical research (ALF), the local Region Skåne County Council, the European Research Council, the Ernhold Lundström Foundation, and Skåne University Hospital.
Disclosure: part of this work has been presented as an abstract during the European Society of Hypertension (ESH) Congress 2023 in Milan, Italy and published in the supplement of Journal of Hypertension: Johansson, Madeleine; Jujic, Amra; Engström, Gunnar; Nilsson, Peter. Increased levels of advanced glycation end products are associated with higher aortic stiffness in younger individuals of the general population. Journal of Hypertension 41 (Suppl. 3): p. e269, June 2023. DOI: 10.1097/01.hjh.0000941784.85947.c4.
Conflicts of interestThere are no conflicts of interest.
REFERENCES 1. Van Bortel LM, Laurent S, Boutouyrie P, Chowienczyk P, Cruickshank JK, De Backer T, et al. Artery Society, European Society of Hypertension Working Group on Vascular Structure and Function, European Network for Noninvasive Investigation of Large Arteries. Expert consensus document on the measurement of aortic stiffness in daily practice using carotid-femoral pulse wave velocity. J Hypertens 2012; 30:445–448. 2. Angoff R, Mosarla RC, Tsao CW. Aortic stiffness: epidemiology, risk factors, and relevant biomarkers. Front Cardiovasc Med 2021; 8:709396. 3. Goldin A, Beckman JA, Schmidt AM, Creager MA. Advanced glycation end products: sparking the development of diabetic vascular injury. Circulation 2006; 114:597–605. 4. Stirban A, Gawlowski T, Roden M. Vascular effects of advanced glycation endproducts: clinical effects and molecular mechanisms. Mol Metab 2014; 3:94–108. 5. Pan J, Bao X, Goncalves I, Jujic A, Engstrom G. Skin autofluorescence, a measure of tissue accumulation of advanced glycation end products, is associated with subclinical atherosclerosis in coronary and carotid arteries. Atherosclerosis 2022; 345:26–32. 6. Deluyker D, Evens L, Bito V. Advanced glycation end products (AGEs) and cardiovascular dysfunction: focus on high molecular weight AGEs. Amino Acids 2017; 49:1535–1541. 7. Luevano-Contreras C, Chapman-Novakofski K. Dietary advanced glycation end products and aging. Nutrients 2010; 2:1247–1265. 8. Fu MX, Wells-Knecht KJ, Blackledge JA, Lyons TJ, Thorpe SR, Baynes JW. Glycation, glycoxidation, and cross-linking of collagen by glucose. Kinetics, mechanisms, and inhibition of late stages of the Maillard reaction. Diabetes 1994; 43:676–683. 9. Zieman S, Kass D. Advanced glycation end product cross-linking: pathophysiologic role and therapeutic target in cardiovascular disease. Congest Heart Fail 2004; 10:144–149. 10. Kass DA, Shapiro EP, Kawaguchi M, Capriotti AR, Scuteri A, deGroof RC, Lakatta EG. Improved arterial compliance by a novel advanced glycation end-product crosslink breaker. Circulation 2001; 104:1464–1470. 11. van Waateringe RP, Fokkens BT, Slagter SN, van der Klauw MM, van Vliet-Ostaptchouk JV, Graaff R, et al. Skin autofluorescence predicts incident type 2 diabetes, cardiovascular disease and mortality in the general population. Diabetologia 2019; 62:269–280. 12. Birukov A, Cuadrat R, Polemiti E, Eichelmann F, Schulze MB. Advanced glycation end-products, measured as skin autofluorescence, associate with vascular stiffness in diabetic, prediabetic and normoglycemic individuals: a cross-sectional study. Cardiovasc Diabetol 2021; 20:110. 13. Llaurado G, Ceperuelo-Mallafre V, Vilardell C, Simo R, Gil P, Cano A, et al. Advanced glycation end products are associated with arterial stiffness in type 1 diabetes. J Endocrinol 2014; 221:405–413. 14. Watfa G, Soulis G, Tartagni E, Kearney-Schwartz A, Borghi C, Salvi P, et al. Relationship between tissue glycation measured by autofluorescence and pulse wave velocity in young and elderly nondiabetic populations. Diabetes Metab 2012; 38:413–419. 15. Choi LS, Ahmed K, Kim YS, Yim JE. Skin accumulation of advanced glycation end products and cardiovascular risk in Korean patients with type 2 diabetes mellitus. Heliyon 2022; 8:e09571. 16. McNulty M, Mahmud A, Feely J. Advanced glycation end-products and arterial stiffness in hypertension. Am J Hypertens 2007; 20:242–247. 17. Ueno H, Koyama H, Tanaka S, Fukumoto S, Shinohara K, Shoji T, et al. Skin autofluorescence, a marker for advanced glycation end product accumulation, is associated with arterial stiffness in patients with end-stage renal disease. Metabolism 2008; 57:1452–1457. 18. McIntyre NJ, Fluck RJ, McIntyre CW, Fakis A, Taal MW. Determinants of arterial stiffness in chronic kidney disease stage 3. PLoS One 2013; 8:e55444. 19. Strozecki P, Kurowski R, Flisinski M, Stefanska A, Odrowaz-Sypniewska G, Manitius J. Advanced glycation end products and arterial stiffness in patients with diabetic nephropathy and patients with chronic kidney disease without diabetes. Pol Arch Med Wewn 2013; 123:609–616. 20. Mac-Way F, Couture V, Utescu MS, Ignace S, De Serres SA, Loignon RC, et al. Advanced glycation end products, aortic stiffness, and wave reflection in peritoneal dialysis as compared to hemodialysis. Int Urol Nephrol 2014; 46:817–824. 21. Linkens AM, Eussen SJ, Houben AJ, Kroon AA, Schram MT, Reesink KD, et al. Habitual intake of dietary advanced glycation end products is not associated with arterial stiffness of the aorta and carotid artery in adults: the Maastricht Study. J Nutr 2021; 151:1886–1893. 22. Mayer O, Gelzinsky J, Seidlerova J, Materankova M, Mares S, Svobodova V, et al. The role of advanced glycation end products in vascular aging: which parameter is the most suitable as a biomarker? J Hum Hypertens 2021; 35:240–249. 23. Mayer O, Seidlerova J, Filipovsky J, Vagovicova P, Wohlfahrt P, Cifkova R, et al. Soluble receptor for advanced glycation end products and increased aortic stiffness in the general population. Hypertens Res 2016; 39:266–271. 24. Gelzinsky J, Mayer O Jr, Seidlerova J, Materankova M, Mares S, Kordikova V, et al. Serum biomarkers, skin autofluorescence and other methods. Which parameter better illustrates the relationship between advanced glycation end products and arterial stiffness in the general population? Hypertens Res 2021; 44:518–527. 25. Brunkwall L, Jonsson D, Ericson U, Hellstrand S, Kennback C, Ostling G, et a
Comments (0)