
Remember me
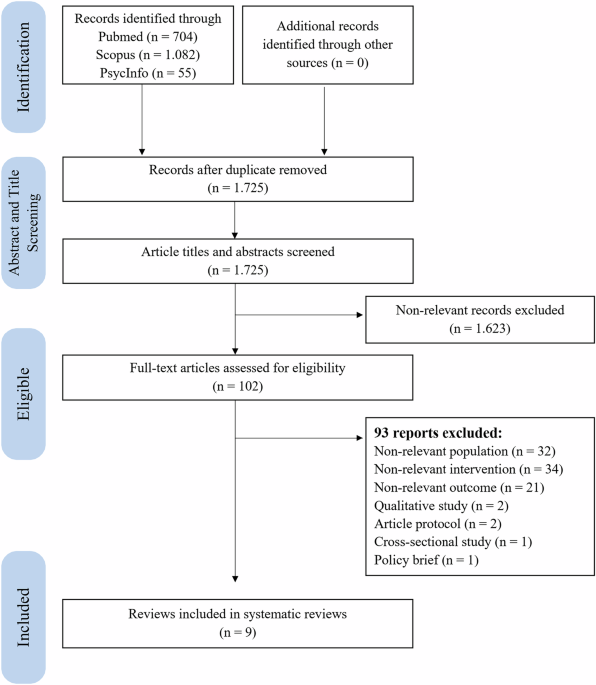

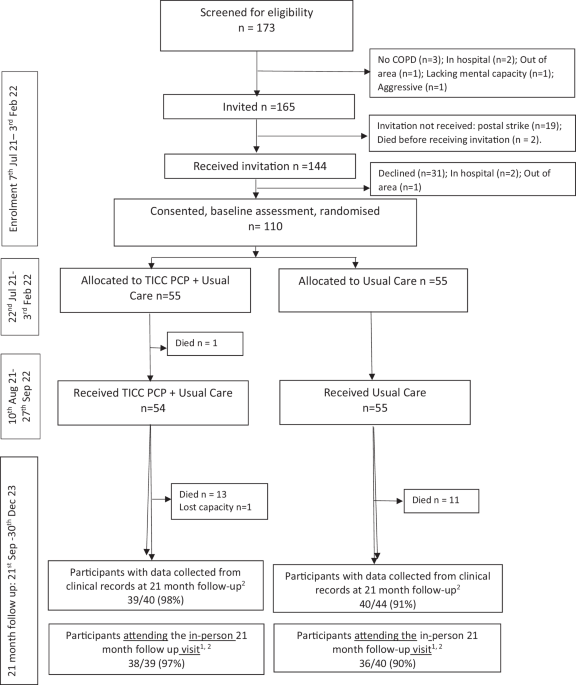
The study selection process adhered to the PRISMA 2020 guidelines, as illustrated in Fig. 1. The initial systematic search yielded 704 records from PubMed, 1082 from Scopus, and 55 from PsycInfo, resulting in a total of 1841 articles. After removing 116 duplicates, 1725 records were available for screening. Title and abstract screening were conducted by one reviewer (IAAP), with a random 10% sample independently reviewed by a second reviewer (VDD), resulting in 100% agreement. Thus, 1623 records were excluded because they were irrelevant to either TPT initiation or psychosocial interventions, leaving 102 articles for full-text review. Of these, 93 articles were excluded for the following reasons: 32 did not meet the population criteria (e.g., they focused on individuals with TB disease or drug-resistant TB); 21 reported outcomes unrelated to TPT (e.g., uptake of tuberculin screening or IGRA tests); 34 articles involved interventions that did not align with the operational definition of psychosocial intervention; 2 articles were solely qualitative assessments of barriers in TPT uptake without evaluating interventions; 2 articles were study protocols; 1 article was a cross-sectional study on the TPT uptake rate; and 1 was a policy brief. Finally, nine studies met all the inclusion criteria and were included in further analysis.
Fig. 1
Flow diagram of the study selection.
Characteristics of the included studiesThe included studies encompass a diverse range of geographic areas and intervention activities, underscoring the widespread recognition of psychosocial interventions as determinants in initiating TPT (Table 1). Among the nine studies, seven (77.8%) were conducted in high TB burden (HTB) countries, including three studies in lower-middle-income (LMI) countries (Ethiopia32, Lesotho33, and El Salvador34) and four in upper-middle-income (UMI) countries (Peru35,36,37, Namibia38). The remaining two studies (22.2%) were conducted in high-income countries (HIC) with low TB burdens (LTB) (Canada39 and the Netherlands40). In terms of study design, five studies34,35,37,38,39 employed an uncontrolled pre-post design, one study32 implemented comparative pre-post designs with concurrent controls, two studies33,36 conducted randomized controlled trials (RCTs), and one study40 employed a mixed-methods implementation approach.
Table 1 Characteristics and outcomes of the included studies.Models of psychosocial interventionAll studies included in this review involved various psychosocial interventions, which were categorized into four categories: (1) health education only34,38; (2) material support along with psychological counseling, home visits, and community workshops35; (3) material support combined with community-based support and home visits36,37; and (4) household-based outreach integrated with health education sessions32,33,39,40. For intervention targets, seven studies (77.8%) targeted people with LTBI, such as household contacts of TB patients32,33,34,35,36,37 and PLHIV38. Two studies (22.2%) focused on broader community groups: one targeted residents in areas with high TB incidence rates, while the other specifically addressed high-risk migrant populations39,40.
These psychosocial models were delivered via a variety of intervention formats. Community-based delivery was the predominant approach (66.7%), highlighting the importance of reaching participants directly within their living environments33,35,36,37,39,40. Magumba et al.38 focused solely on interventions in clinical settings, whereas two studies (22.2%) employed a combined approach that integrated clinical interventions with household outreach, helping to reach more family members and foster greater community engagement33,34.
The educational content of these psychosocial interventions covered a variety of essential topics related to TB. The most frequently addressed themes included the following: benefit, regimens, duration of TPT (88.8%)32,33,34,35,36,38,39,40, TB transmission (33.3%)34,36,39, TB symptoms and LTBI awareness (n = 2, 22.2%)34,39, treatment adherence (33.3%)33,34,35, potential side effects (22.2%)34,38, LTBI common misconceptions (22.2%)34,39, and survivor testimonials to motivate participants (44.4%)34,35,36,40. Rocha et al.35 and Wingfield et al.36 enhanced educational support by providing financial management during TB care. Additionally, Rocha et al.35 empowered communities through mobilization workshops that offered training on how to register for health insurance and guidance on income-generating skills. Educational materials were presented in audiovisual formats (33.3%)34,39,40, printed materials (22.2%)33,38, and verbal presentations during workshops and home visit descriptions (44.5%)32,35,36,37.
In addition to health education, six studies (66.6%) provided targeted psychological and social support, which included structured counseling for managing depression35, strategies to reduce community TB-related stigma34,35,36,40, and emotional support to encourage treatment adherence32,37. Efforts to reduce stigma have been made through various methods, such as short films featuring local community figures39,40, testimonies from TB survivors in regional languages to increase community engagement34,39 and peer support35,36. All the included articles (100%) utilized multisession methods over several months, promoting ongoing engagement and supporting the successful initiation and completion of TPT. The longest intervention lasted 34 months, although detailed information regarding the specific number or duration of sessions was reported inconsistently across the studies.
Intervention providersThe psychosocial interventions in four studies (44.4%) involved helper-guided approaches featuring either multidisciplinary healthcare professionals alone34,35,36,38 or a combined model of multidisciplinary healthcare professionals and community health workers (55.6%)32,33,37,39,40. The multidisciplinary healthcare teams, which include physicians, psychologists, nutritionists, and TB nurses, work primarily in clinical or structured outreach settings. Their duties included clinical examination, diagnosis, monitoring of adverse events, providing nutritional and financial support, and training CHWs. The CHWs included health extension workers (HEWs), village health workers, women-led community associations, and community health workers linked with NGOs. They were responsible for conducting household visits, providing peer education, mobilizing the community, screening for symptoms, offering psychological and emotional support, reducing stigma, facilitating healthcare referrals, and delivering ongoing support to encourage treatment adherence.
Quality of the included studiesThe total CCAT scores ranged from 37.5–85% (Supplementary Material Table 2). Three studies were classified as high quality33,36,37, five as moderate quality32,34,35,39,40 and one as low quality38. The studies indicated that the preliminaries had the highest average score of 5.0, followed by the introduction at 4.78. This reflects consistent clarity in framing, structured abstracts, and well-articulated rationales for the studies. In contrast, the most frequently underperforming domains were design (2.33), sampling (2.78), and data collection (2.78), highlighting methodological weaknesses.
The low average score in the design domain stemmed from a lack of control groups in six studies (67%), which limited causal inference34,35,37,38,39,40. Additionally, four studies (44%) did not report whether concurrent changes in the National Tuberculosis Programs (NTPs) had any influence on outcomes. Additionally, three studies (33.0%) failed to provide details on the educational content offered. They did not clarify the intensity or frequency of psychosocial counseling or home visits, which are essential for assessing implementation fidelity. None of the studies included reported on sample size calculations or provided statistical justification for their sampling methods. This weakness undermines the assessment of whether the study was sufficiently powered to detect meaningful differences in outcomes.
In the data collection domain, two studies relied only on project-based records, which are more prone to measurement bias39,40. In contrast, seven studies utilized routine health facilities or national database systems32,33,34,35,36,
Comments (0)