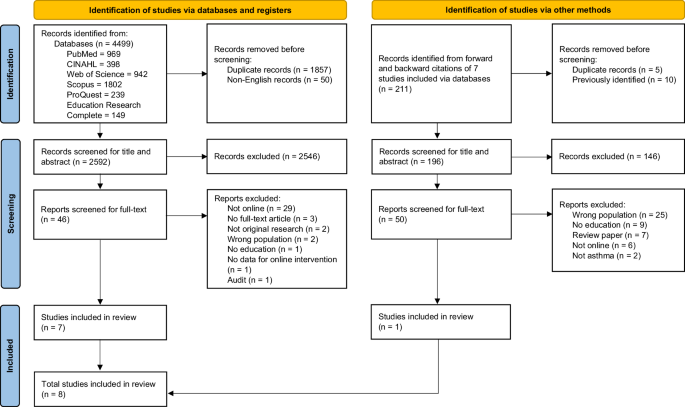
This systematic review identified eight studies examining online asthma training programmes for school staff, conducted between 2011 and 202332,33,34,35,36,37,38,39. All included studies were from high-income countries and focused on immediate knowledge gains. The overall quality of the included studies varied, with only two studies rated as high quality33,37, which is an important consideration when interpreting the findings. All studies demonstrated significant knowledge improvements in effect size with more than 50% reporting medium to large effect sizes (Cohen’s d range: 0.537–3.409). Furthermore, direct comparisons between online and face-to-face formats found no significant difference in learning outcomes32,39. However, none evaluated longer-term behavioural or organisational outcomes, representing a critical evidence gap.
The positive outcomes observed at Kirkpatrick levels 1 and 2 establish a foundation for effective online asthma training32,33,34,35,36,37,38,39. The improvement in knowledge scores and high satisfaction ratings indicate that participants found the training relevant and engaging. These findings align with evidence from other fields, such as virtual training in nursing and sexual health education, where participants reported increased knowledge and satisfaction with e-learning content40,41. This is particularly important in the school context, where school staff often have limited time for professional development and may feel unprepared to manage students with asthma8. The inclusion of self-efficacy measures in some studies further supports the idea that participants not only gained knowledge but also felt more confident in their ability to respond to asthma emergencies32,35,38,39. The training programmes covered a wide range of topics, including asthma pathophysiology37,39, symptom identification32,33,34,35,36,37,38,39, medication use32,33,34,35,36,37,38,39, and provision of first aid for asthma32,33,35,36,37,38,39, which reflects a comprehensive approach to asthma education. However, the use of scenario-based assessments in several studies suggests that knowledge alone may be insufficient for effective real-world application32,33.
A key issue in the current evidence is the variation in how asthma knowledge was assessed. For instance, the NAKQ includes open-ended questions that may be too complex for school staff, potentially limiting its suitability36. Several studies used self-developed questionnaires, which were not validated34,35. While these tools may be tailored to the training content, the lack of standardisation makes it difficult to compare results across studies and ensure accurate measurement of knowledge change. Developing validated instruments specifically for school staff would allow for more consistent evaluation of training outcomes.
Although knowledge gain is essential, true impact depends on demonstrating safer practices (level 3) and organisational improvements (level 4). The predominance of single-group designs33,34,35,36,37,38 and lack of long-term follow-up32,33,34,35,36,38,39 make it impossible to assess real-world applications or school health improvements. Level 3 evaluations are achievable, as demonstrated in other health studies, through methods such as long-term follow-up with supervisor observations, participant self-reports, or workplace audits40,42,43. Similarly, level 4 impacts have been documented when public health courses led to institutional policy changes44. The lack of level 4 outcomes is concerning, as schools need evidence of organisational benefits to support the continued implementation of training programmes. Potential level 4 outcomes might include reduced asthma-related school absenteeism, fewer hospitalisation and emergency visits, and a decrease in days with interrupted activities due to asthma45,46. Face-to-face school asthma programmes were found effective for these outcomes47. However, online programme lacks such evidence, and it becomes challenging for schools to justify spending time and resources on these programmes, which may hinder their adoption and sustainability. None of the included studies reported cost-effectiveness comparisons between online and face-to-face training. Such data could help schools make informed decisions, especially given that online training is likely to be more cost-effective and less labour-intensive when implemented on a larger scale. While these assessments require more resources, they provide the most meaningful evidence of training effectiveness48.
Online training programmes offer several practical benefits for school settings. Its broad accessibility, cost-effectiveness, standardised content delivery, and the flexibility of self-paced learning make it a feasible option for school staff who often struggle to find time for professional development49. The two included studies that directly compared delivery modalities, such as online versus face-to-face, or synchronous versus asynchronous formats, reported no significant difference in learning outcomes32,39. Therefore, based on this limited evidence, it can be assumed that online training programmes were not inferior to face-to-face training approaches. However, online formats still fall short in providing the hands-on experience, peer interaction, and real-time feedback that in-person training can offer22. This also highlights the importance of considering technological access, such as reliable internet access, availability of digital devices, and adequate digital literacy, when planning online interventions, which could be significant barriers in LMICs50. A pragmatic approach is a hybrid model, using online modules for foundational knowledge and refreshers, complemented by targeted in-person sessions to reinforce skills51.
In terms of the design of the online interventions, among the four studies using the web-based modules, those that used a combination of videos, voice-over slides, quizzes, and scenario-based learning, showed greater knowledge improvements33,34,35. Francisco’s Teaming Up for Asthma Control (TUAC) programme achieved the highest knowledge improvement (84.73%), likely due to its focused content, alignment with state policy, and contextual relevance to local school needs34. In contrast, Nowakowski’s Asthma 101 programme showed small knowledge gain (5.33%)37. The programme covered broader foundational topics but reused similar slide content from the in-person training. In addition, participants already had a high level of baseline knowledge, which likely contributed to the limited knowledge gain37. This suggests that simply transferring traditional teaching materials into an online format is insufficient without attention to engagement and content relevance52.
There are several limitations to this systematic review. First, only eight studies met the inclusion criteria, and all were conducted in the USA and Australia, which limits the generalisability of the findings to other cultural and educational contexts. Secondly, the review included only English-language publications, potentially excluding relevant non-English studies. Thirdly, many studies have a small sample size and lack complete statistical reporting, particularly standard deviations required for calculating effect sizes, and attempts to obtain this information from authors were largely unsuccessful33,34,37. Finally, a meta-analysis was not feasible due to significant heterogeneity in study designs, outcome measures, and intervention formats, which led us to adopt a narrative synthesis approach30.
Implications for practice and future research
Despite evidence gaps, consistent knowledge gains across online formats suggested that schools can adopt online asthma training for school staff. A hybrid approach may offer the most practical solution, offering the strengths and limitations of both modalities. Regardless of the delivery method, effective training should align with school policies, emergency plans, and strong partnerships with healthcare providers and families8,53.
Future studies should (i) use robust designs (e.g., RCTs), (ii) include 3–6-month follow-up with behavioural measures (level 3) and school-level outcomes (level 4), (iii) employ validated, school-appropriate instruments with standardised reporting tied to Kirkpatrick levels, and (iv) incorporate implementation and economic evaluations to inform scale-up54. Current studies often focus only on knowledge retention and programme satisfaction, which may not show real-world effectiveness.


Comments (0)