Statement of principal findings
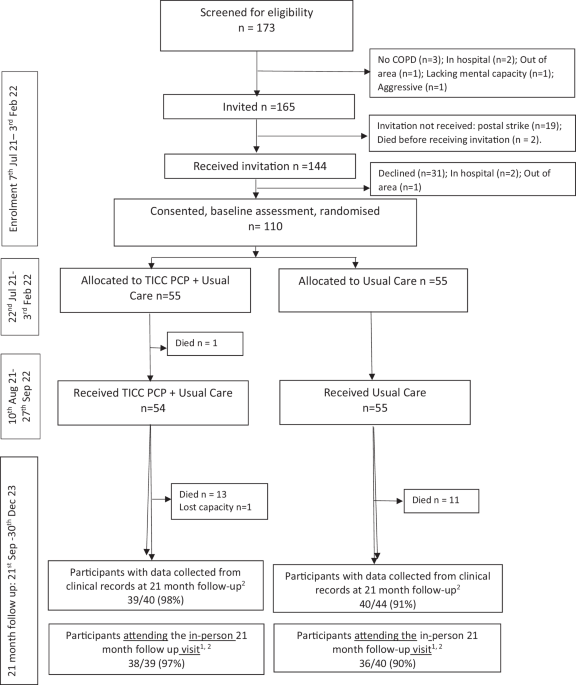
Recruitment, retention, and data collection targets were achieved as planned (or with slight modifications). One quarter of TICC-PCP intervention participants received at least the planned monthly (first six months) then bi-monthly (subsequent six months) contacts: they received almost double the expected number of home visits. The remainder received nine contacts, on average, suggesting the flexibility of TICC-PCP visits led to tailoring by Pharmacists according to participants’ needs.
A multimorbid cohort (mean of 11.5 (SD 6.9) conditions at baseline) received an increasing number of daily medicines over time.
Pharmacists built trusting therapeutic relationships, overcoming challenges to in-person contact during the COVID-19 pandemic. They conducted clinical assessments and prescribed a range of medicines in collaboration with consultant respiratory physicians and wider teams. Intervention arm participants appeared less likely to use rescue packs for exacerbations and attend emergency care or hospital for respiratory reasons although the duration of hospitalisation (for any reason) was longer for intervention arm participants. This latter observation appears at odds with the rest of the findings and requires further exploration in a definitive trial. A signal of longer duration of hospitalisations suggests participants admitted to hospital from the intervention arm were sicker than participants in the UC arm. The optimal time to detect any apparent improvement in outcomes appeared to be 12 months (end of intervention), which has implications for designing a subsequent definitive trial.
There were signs that health related quality of life, anxiety and depression and treatment burden outcomes favoured the intervention arm as compared with the UC arm during the one year intervention, without any apparent increase in primary care GP contacts.
The need for a subsequent definitive trial is supported by a parallel qualitative process evaluation in which participants (particularly those living in more socioeconomically deprived areas) and staff were supportive of the TICC-PCP approach25. In such a trial, if the primary outcome is the number of participants with Emergency Department attendance at 12 months and we observe a proportion attending the Emergency Department in UC of 0.325, and the proportional improvement in TICC-PCP vs UC was 0.125, the estimated sample size per arm with data would be 208 with 80% power.
Strengths and weaknesses
Strengths included detailed participant and service utilisation data, recruitment and follow up processes, a reasonable period of follow up, good description of the intervention and detailed changes made by pharmacists. Unlike previous studies of this type26,27,28, where Pharmacists with additional respiratory therapeutics training delivered care in clinics, focusing on the single morbidity of respiratory disease, offering support for inhaler technique and advice on swift management of exacerbations, the TICC-PCP pharmacists were generalists. Given that most pharmacists are generalists, we suggest this is likely to aid implementation, while helping to address co-morbidities, many of which worsen quality of life in patients with COPD.
The collaborative, integrated intervention involving consultant respiratory physicians ensured safe practice and clinical governance.
Weaknesses included uncertainty on the typology of participants most likely to benefit from TICC-PCP, and, while the majority of participants lived in the most socioeconomically deprived Scottish areas, there was a noted lack of ethnic diversity. In a future RCT, consideration can be given to modifying recruitment to increase uptake in minority ethnic groups and people who struggle to attend out patient appointments e.g. people experiencing homelessness. Subgroup analyses could identify those who experience greatest gain.
Uncertainty as to the magnitude of the positive Hawthorne effect of three monthly home visits by researchers could be overcome if outcome data were collected through remote record linkage. This approach may also facilitate identification of cause of death. Enrolment and the first four months of TICC PCP delivery also overlapped with COVID-19 lockdown when much community based research was paused, however our trial steering group made the decision to continue the study, with researchers donning and doffing protective clothing and equipment, given the potential benefits of home visits to otherwise isolated, housebound participants.
Interpretation in context of published literature
RCTs of HCP-led interventions for people with COPD focused on specific respiratory issues e.g. medicine adherence/inhaler technique, rather than addressing comorbidities and wider health determinants29,30,31,32,33,34. Pharmacist prescriber led home visits remain untested in this and other therapeutic areas29,30,31,32,33,34. Definitive trials assessing outcome measures other than HRQoL are lacking29,30,31,32,33,34. Three systematic reviews (two focused specifically on pharmacist interventions/care) reported that the available evidence lacked robustness26,27,28. Two underscored the importance of monitoring and reporting variations in UC over time, as we have done27,28. The wider evidence base for pharmacist medication review in the UK is marked by two studies, both of which involved low intensity interventions, and neither of which showed improved outcomes13,35. In the HOOPS, pharmacists visited people with Left Ventricular Systolic Dysfunction (LVSD) in their homes or General Practices, conducting medicine reviews that were similar to those delivered by TICC-PCP pharmacists, although the latter prescribed autonomously while HOOPS pharmacists made recommendations to GPs for medicine changes. The HOOPS failed to reach the primary end point (death/hospitalisation for heart failure), despite improvements in the prescribing of evidence based disease modifying treatments for LVSD.
In the HOMER RCT, two home visits by pharmacists (non prescribers) to elderly patients receiving polypharmacy post discharge, was associated with a significantly higher rate of hospital admissions and did not improve quality of life. GP home visits increased, and there was a statistically insignificant increase in deaths in the control group35. While we did not observe the former, there were more deaths in the TICC-PCP arm.
Deprescribing interventions have been the focus of much research over the past 20 years, however, trials are generally of short duration (less than one year) and clinical and health service outcomes have not been comprehensively assessed36. As far as we are aware, IP Pharmacist led deprescribing has not been explored as a means of reducing falls or emergency department visits, and the impact on patients remains unclear.
Generalist Pharmacy technicians are capable of undertaking many of Pharmacists’ traditional roles including some of those enacted by pharmacists in the TICC-PCP intervention, raising the question of whether pharmacy technicians could offer a more affordable approach37.
Pharmacists commonly made clinical guideline based changes to medicines in one or more of the seven categories described in Table 5. There was no overall signal of Pharmacists having de-prescribed to a greater extent than UC (mean number of medicines increased in both groups) although deprescribing was observed in relation to medicines for anxiety and depression. Respiratory interventions were the most common, and possibly contributed to the pattern of fewer unscheduled care attendances. A subsequent definitive RCT is needed to test this hypothesis.
Home visits and protocol led changes to the defined range of medicines identified in this study could be undertaken by healthcare professionals with less advanced training than independent prescriber pharmacists. For example, Pharmacy Technicians could provide the relationship based pharmaceutical care valued by participants, while achieving similar outcomes at lower cost, enabling long-term sustainability. Such a trial could target people with COPD and co-morbidities who struggle to access primary care, e.g. people experiencing homelessness, who have a disease and treatment burden in excess of those shown by participants in the present study, and are less likely to receive medicines for COPD12. Alternatively, the target group could be people with higher rates of emergency healthcare use where COPD is among the principal causes, e.g. people using illicit opioids38.
The observed improvements in HRQoL, anxiety, depression and treatment burden in the intervention arm relative to UC, were achieved despite signs that the intervention led to a decrease in medicines for anxiety and depression in the intervention arm relative to UC. It is possible that the frequent (nine visits over a year) healthcare professional home visits to people who are increasingly breathless at rest and housebound, provided reassurance while expediting access to consultant respiratory physician advice. Findings from the parallel qualitative process evaluation support the idea that the relational aspect of the visits were highly valued by participants who are increasingly co-morbid with limited mobility25.
Baseline utility scores and health state utilities were lower than the values reported in other cross-country settings39 and studies of other long-term conditions40. Reasons for this are unclear, but the extent of socioeconomic disadvantage and number of comorbidities may be contributory41.


Comments (0)