
Remember me

Eosinophilic asthma represents a distinct inflammatory phenotype characterised by increased eosinophilic airway inflammation, often associated with corticosteroid responsiveness and increased exacerbation risk. The identification of eosinophilic asthma in clinical practice is increasingly guided by blood eosinophil counts (EOS)1,2, but fractional exhaled nitric oxide (FeNO) has been proposed as a complementary non-invasive biomarker3. One such multi-component framework was proposed by the International Severe Asthma Registry (ISAR) that incorporates both biomarkers to better identify eosinophilic phenotypes across the asthma severity spectrum4. Despite the recognized burden of mild asthma at the population level, few validated frameworks exist to classify inflammatory phenotypes in this group. Although GINA now recommends ICS-containing therapy in all asthmatics, evidence suggests that responses may differ: non-eosinophilic patients can respond better to tiotropium, and the majority of mild asthmatics are non-eosinophilic5,6. Inflammatory phenotypes were originally defined using sputum eosinophils but given the impracticality of sputum testing in large cohorts, blood eosinophils and FeNO have emerged as feasible, scalable biomarkers to guide phenotyping in both clinical and epidemiological settings.
We therefore explored whether a simplified version of the ISAR algorithm, originally developed for severe asthma, could be meaningfully adapted for use in a population-based mild asthma cohort. The ISAR algorithm incorporates key systemic features (oral corticosteroid use and asthma onset) which were unavailable in our cohort. We thus evaluated a simplified classification approach based on ISAR-derived biomarkers (EOS, FeNO, and nasal polyps). This adaptation reflects milder disease constraints where systemic manifestations are fewer, and inflammation may be less clinically overt.
In particular, we evaluated whether the incorporation of FeNO into the ISAR-based algorithm improves the multicomponent classification of eosinophilic asthma in those with presumed mild disease in the Austrian LEAD (Lung, hEart, sociAl, boDy) study cohort (clinicaltrials.gov identifier: NCT1727518)7. 708 adults (≥18 years) had a prior asthma diagnosis; 32 of whom had invalid spirometry, 221 with missing FeNO and/or EOS measurements; and 4 with invalid FeNO and/or EOS measurements- participants with missing EOS, FeNO, or valid lung function measurements were excluded. Diagnosis of nasal polyps were self-reported. Asthma phenotype was graded using the ISAR algorithm, with and without FeNO as a criterion. Both models (EOS+FeNO vs. EOS-only) were fitted on the same analytical cohort of 451 individuals, with eosinophilic phenotype (Grade 2/3) defined using either eosinophils alone or in combination with FeNO. While the EOS+FeNO model included additional biomarker input, both models predicted the same binary outcome (Grade 0/1 vs. Grade 2/3). Model performance was assessed using fit indices (Akaike information criterion, AIC, and Bayesian information criterion, BIC), Cohen’s κ and calibration indices (Breier scores, slope, intercept, optimism-corrected C-statistics and R2, and maximum calibration error [Emax]) were additionally confirmed visually by calibration plots8. The predictive performance of two logistic modes for both models were evaluated with internal validation using 500 bootstrap resamples.
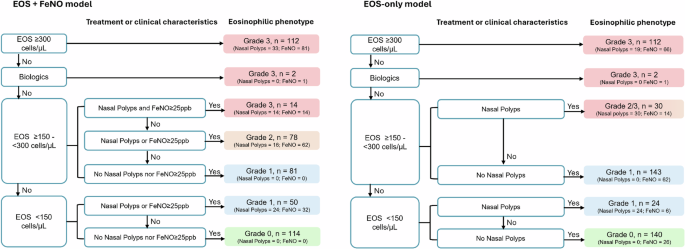
The EOS+FeNO model reclassified 13.7% more individuals into the eosinophilic (Grade 2/3) phenotype (45.7% vs. 32.0%, McNemar’s p < 0.001; Fig. 1). While the eosinophilic phenotype was still apparent in mild asthma, proportions were much smaller compared to severe asthma cohorts (ranging between 72.6% to 92.1%)4,9. The inclusion of FeNO substantially improved model fit (AIC: 117.6 vs. 181.3; BIC: 134.1 vs. 193.6) and discrimination (C-statistic: 0.986 vs. 0.945) when asthma status was regressed on eosinophil and FeNO levels. FeNO additionally improved explanatory power with a higher optimism-corrected R2 (0.916 vs. 0.807) and a lower Brier score (0.031 vs. 0.060). Calibration curves (Supplementary Data 1) indicated that both models were well-calibrated with small maximum calibration errors (Emax: 0.031 and 0.025 respectively). However, the EOS+FeNO model exhibited near-ideal calibration (intercept: 0.068 and slope: 1.095), while the EOS-only model showed slight underfitting (intercept: –0.052 and slope: 0.929). These findings suggest that FeNO meaningfully enhances both the accuracy and reliability of risk prediction for asthma beyond eosinophils alone.
Fig. 1: Flowchart based on an adapted ISAR-based criteria showing the prevalence of non-eosinophilic and eosinophilic phenotypes in models with (left) and without (right) fractional exhaled nitric oxide (n = 451).
The sample sizes of each grade are shown text in figure together with the prevalence of individuals with nasal polyps or FeNO ≥25ppb. EOS, eosinophil; FeNO, fractional exhaled nitric oxide.
Importantly, agreement between models was substantial (Cohen’s κ: 0.716), with similar demographic and clinical distributions across classification. Those with an eosinophilic phenotype (Grade 2/3) were more likely to be males, and generally have higher values of body composition, IgE levels, but have a smaller proportion of those with well-controlled asthma, negligibly lower lung function and reported a higher use of Inhalative than those with a non-eosinophilic phenotype in both models (Table 1). The additional reclassification observed with the inclusion of FeNO was not attributable to demographic or clinical confounding but likely reflects added discriminatory capacity of FeNO in detecting airway inflammation that was not captured by blood eosinophils alone.
Table 1 Demographics and clinical characteristics in asthma categorised by the modified ISAR-based gradient (with and without FeNO).Since the majority of our cohort was steroid (inhaled corticosteroids/long-acting beta-agonists)-naïve- a group in whom eosinophilic inflammation is most informative for guiding first-line therapy- a dedicated subanalysis was additionally performed. 41.5% of steroid- naïve individuals were classified as eosinophilic (Grade 2/3) in the EOS+FeNO model compared with 27.1% using EOS alone (reclassification of 14.4%, McNemar’s p < 0.001; Supplementary Data 2). Discrimination (C-statistic: 0.978 vs. 0.888) and explained variation (R²: 0.932 vs. 0.807) were higher for EOS+FeNO, with calibration near-ideal (slope 1.011, intercept 0.001) despite elevated Emax due to small sample sizes. This aligns with general population findings but highlights that even in steroid-naïve asthma, FeNO detects airway inflammation missed by EOS alone. While previous studies in mild steroid-naïve asthma reported limited added value of FeNO over blood eosinophils for sputum eosinophilia10, our findings suggest that FeNO remains a pragmatic, point-of-care complement to blood eosinophils for airway inflammation in this population. Integrating FeNO into routine phenotyping could help identify ICS-responsive patients while avoiding unnecessary treatment in non-eosinophilic individuals, who may respond better to alternative therapies such as tiotropium5,6.
These findings raise key considerations for the use of FeNO in phenotyping mild asthma. First, systemic eosinophilia and airway inflammation are not always concordant in mild disease where inflammation is often intermittent or subclinical11. Integrating FeNO with eosinophils yields more accurate, better-calibrated classification even in a predominantly mild cohort. This is supported by the modest improvements in model fit and calibration when FeNO was added. These findings are consistent with the known biology of FeNO, which captures local Type 2 (T2)-driven airway inflammation that may not be reflected systemically, especially in the early course of asthma12.
Although the addition of FeNO modestly improved model performance, some reclassification may reflect biomarker variability rather than stable phenotypic shifts. While EOS is not a definitive gold standard in clinical assessments of asthma, EOS remains a widely used and guideline-supported biomarker in both research and clinical settings. FeNO, by contrast, reflects T2-driven airway inflammation and is more susceptible to variation due to atopy, allergen exposure, or recent environmental triggers—factors that can vary independently of asthma control or severity3,13. Additionally, both FeNO and EOS levels are modified by smoking, which can obscure biomarker interpretation14,15,16. These characteristics may limit the reliability of FeNO as a stable standalone classifier in cross-sectional population settings. Instead, FeNO may identify transient or localised T2-driven inflammation, thereby improving classification in these select individuals missed by systemic biomarkers. Supporting this, total IgE levels were significantly higher in individuals classified as eosinophilic (Grade 2/3) across both models, suggesting an underlying atopic component consistent with T2 inflammation. However, the cross-sectional design limits our assessment of seasonal or temporal variations. Nonetheless, these findings raise the possibility that FeNO may reflect temporary rather than persistent airway inflammation, underscoring the need to interpret FeNO within clinical context—ideally in conjunction with longitudinal data3,9.
Secondly, while gradient-based classification systems like ISAR have demonstrated utility in severe asthma4,9, their utility in milder disease may be more limited. Although FeNO significantly reclassified individuals, the marginal improvement in discrimination and calibration suggests that this added complexity may not meaningfully impact clinical management in low-risk populations. The inclusion of FeNO likely reflects sensitivity to transient or subclinical airway inflammation, which may not translate into meaningful differences in clinical outcomes or management decisions. The increased proportion of individuals classified as eosinophilic when FeNO is added appears to be driven largely by borderline or isolated FeNO elevations and thus may not yield meaningful stratification beyond what dichotomous definitions offer. Indeed, multi-level classifications may overcomplicate phenotyping in a population with few exacerbations, minimal and/or heterogenous symptom burden and instability is high17,18,19. Future research incorporating longitudinal data and outcome measures is needed to clarify whether these reclassifications represent clinically relevant phenotypic shifts or simply biomarker variability.
Our findings align with prior studies showing that FeNO offers limited predicted values for exacerbation risk or clinical outcomes in unselected populations unless considered alongside other clinical features and longitudinal data20,21,22. While FeNO retains clinical value for assessing inhaled corticosteroid responsiveness or monitor adherence1, its role as a standalone classifier in cross-sectional phenotyping of mild asthma appears to be limited. In research and population-level surveillance, FeNO may be best employed as a supplementary biomarker—ideally integrated with longitudinal assessments—rather than as a primary or static classifier. Importantly, FeNO thresholds may not be universally optimal across diverse populations23,24,25. Just as the generalizability of the 300 cells/µL EOS threshold lacks universal applicability26,27, FeNO may also require population-specific calibration, particularly for a mild asthma cohort. Within this context, the steroid-naïve subanalysis here demonstrates that FeNO can meaningfully complement blood eosinophils missed by systemic markers, particularly given its ease of use, non-invasiveness, and repeatability. Altogether, a one-size-fits-all approach to FeNO thresholds may be inappropriate and underscore the need for individualised or population-tailored benchmarks for phenotyping accuracy.
A limitation is that nasal polyps were identified through self-reported medical history, which may be less accurate than physician-confirmed diagnoses and could have affected classification accuracy. A further limitation is the absence of longitudinal biomarker data which precludes the assessment of phenotype stability over time. This impacts clarification whether FeNO captures transient inflammation or reliably reflects a persistent airway eosinophilic endotype.
While the ISAR algorithm was developed for severe asthma and biologic eligibility, phenotyping remains relevant in mild asthma for early identification and treatment guidance. These results demonstrate the FeNO improves classification accuracy and calibration in an adapted ISAR-based phenotyping model for mild asthma but also report that frameworks tailored to severe disease may not translate effectively to milder, population-based cohorts where inflammatory signals are more subtle and clinical outcomes less pronounced. Indeed, the added value may be most relevant for research and surveillance rather than routine clinical application. Future work should focus on dynamic phenotyping incorporating longitudinal biomarker trends, symptom trajectories and treatment response over time.
Comments (0)