
Remember me

A mixed-method study was designed to evaluate the de-implementation strategy to De-implement inappropriate ICS use in COPD patients in the province of Drenthe (DECIDE), the Netherlands. The implementation strategy was evaluated using the Proctor framework27. The Proctor framework is a widely used model for evaluating implementation projects, distinguishing between implementation, service, and client outcomes. The study consisted of three interrelated parts: (1) a retrospective cohort analysis of regional ICS prescription data to assess changes in ICS use over time, serving as the primary outcome; (2) a prospective study in general practices evaluating the safety, effectiveness, and patient satisfaction of ICS withdrawal, while capturing strategy adoption and implementation fidelity; and (3) semi-structured interviews with patients and nurses to explore implementation outcomes and overall satisfaction. Box 1 provides an overview of evaluated outcomes. The study was exempted from ethics review by the medical ethics review board of the Radboud University Medical Center (file number 2021-12394) as it did not fall under the Dutch Medical Research Involving Human Subjects Act.
Box 1 Outcomes assessed in the DECIDE study based on the framework by Proctor27
Data-collection: 1 Part 1: Regional general practice-level data, 2 Part 2: prospective study on ICS withdrawal in patients with Chronic Obstructive Pulmonary Disease (COPD), 3 Part 3: semi-structured interviews of practice nurses and patients.
Regional contextDrenthe is one of the 12 provinces of the Netherlands, with approximately 500,000 inhabitants. All inhabitants of Drenthe receive care from one of the 140 general practices that are part of a regional general practices cooperation (RGPC) called ‘Doctor Drenthe’ (in Dutch: Dokter Drenthe, see www.dokterdrenthe.nl). In 2008, the RGPC launched a health insurer-funded integrated disease management (IDM) program for COPD, supported by dedicated RGPC nurse consultants that assist local general practices with implementation. In 2021, a large group of program-affiliated practices were invited to use the de-implementation strategy and participate in the evaluation study. Recruitment ran from July 2021 to September 2022, with several COVID-19-related delays.
Development of the de-implementation strategy to reduce inappropriate ICS use in COPDWe used the de-implementation guide of the Dutch program “To Do or not to Do” as framework to design our de-implementation strategy28. The step-by-step approach outlined in this de-implementation guide closely aligns with the Grol and Wensing model for implementing change in healthcare and incorporates a determinant framework to support comprehensive problem analysis29. We identified key regional stakeholders (i.e., a patient, chest physician, general practitioner (GP), clinical nurse specialist, practice nurse (PN), psychologist, pharmacist, and representative of the health insurance company) and invited them for one-on-one interviews about potential barriers and opportunities to reduce inappropriate ICS use in patients with COPD. Next, all stakeholders were invited for and participated in a digital stakeholder meeting to prioritize barriers and opportunities to reduce inappropriate ICS use in the region and decide on effective intervention strategies. The project team set up a de-implementation strategy based on the prioritized barriers and facilitators and consensus for the strategy was reached among the stakeholders.
De-implementation strategyThe de-implementation strategy comprised three main elements: a communication plan, training for general practice staff, and a digital toolbox. The communication plan aimed to inform and educate healthcare providers about the project and appropriate use of ICS in COPD management. A number of newsletters, personal outreach, and articles in professional magazines were published to enhance appropriate ICS prescribing practices and reduce inappropriate ICS use in patients with COPD. Additionally, project information was included in regional communication platforms and integrated into several asthma and COPD-related regional training courses to further raise awareness and promote best practices. Video material (in Dutch) was developed to support the implementation.
A training program was developed to help GPs and PNs reduce inappropriate ICS use in COPD, featuring a one-hour in-practice session by RGPC consultants, a digital self-learning version, and follow-up support through at least two consultant contacts.
The toolbox (in Dutch, see eSupplement) was set-up with pre-existing and newly developed information, resources, and tools that general practice health care professionals could use to de-implement inappropriate ICS use in COPD. The toolbox covered key themes like diagnosing asthma and COPD, patient education on medication, appropriate ICS indications, selecting and supervising ICS withdrawal, and criteria for restarting ICS when needed. Examples of the tools that were available in the toolbox were: a decision tree on appropriate inhaler medication use for COPD, a flowchart to help select patients for ICS withdrawal, templates of patient information letters, a questionnaire to evaluate side effects of ICS, and links to informative videos on public websites. The RGPC’s consultants explained how to use the toolkit to GPs and PNs during the educational session.
Data collection and outcomesPart 1. Regional data from integrated disease management for COPDEvery three months data was extracted from the electronic patient journal systems of all general practices that participate in the IDM program for COPD through a regional health information platform (VIPlive, Topicus, the Netherlands). The quarterly reports consisted of information on: the total number of patients with COPD registered with a general practice, the number that participated in the COPD IDM program, respiratory medication use (including ICS use), lifestyle (like smoking status), disease severity (like Forced Expiratory Volume in 1 s (FEV1) as a percentage of predicted value (FEV1%pred), exacerbations, and Clinical COPD Questionnaire (CCQ) scores. These data were aggregated at the practice level for patients who participated in the COPD IDM program and whose participation was claimed from a healthcare insurance company.
Outcomes for ICS useThe quarterly (Q) reports included information on the proportion of patients with current ICS use. Current ICS use is defined as having an ICS prescription issued within the past 28 days or a repeat prescription scheduled in the future, without a documented stop order for ICS within the past 28 days. Due to unforeseen and unavoidable COVID-19 measures at the time, the invitation of COPD patients to discuss ICS withdrawal with their PN was postponed until the first quarter of 2022 (Q1 2022). Current ICS use data collection commenced with the start of these visits, as this variable was included in the IDM dataset on 1 January 2022. Data collection concluded in the second quarter of 2023 (Q2 2023), following the final ICS withdrawal attempt in Q1 2023. Therefore, our analysis covers the period from Q1 2022 to Q2 2023.
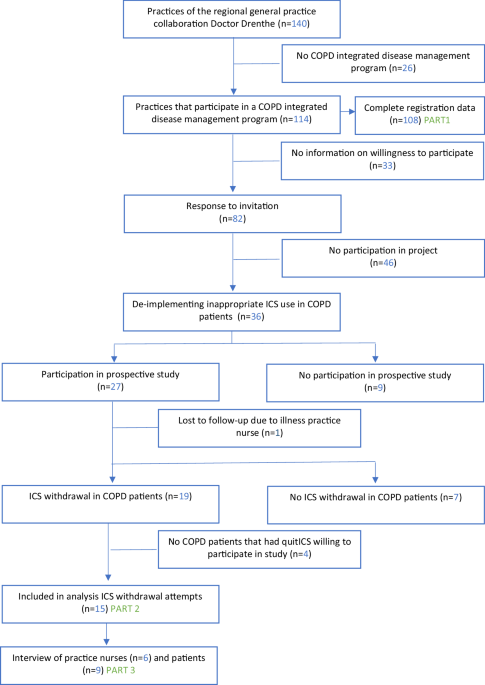
Selection and categorization of general practicesData from general practices was excluded from further analyses if (i) information of more than one quarterly reports was missing; (ii) the practice was new and still building a patient base (<1000 registered patients); or, (iii) the practice had just started with the COPD IDM program. Practices were categorized as (A) fully participated in the prospective evaluation study (part 2), (B) intended to reduce inappropriate ICS use in COPD patients in their practice but incomplete participation in the evaluation study, and (C) other general practices in Drenthe that participate in the COPD IDM program but did not receive or accept our invitation to participate in the study (i.e. ‘passive exposure’ group).
Part 2. Prospective study on ICS withdrawal in COPD patients in general practicesData on ICS withdrawals in patients with COPD during the study period were collected from the participating general practices classified in Group A (full participation). A practice was considered to have fully participated if it met all of the following criteria: (i) agreement to take part in both the DECIDE program and the evaluation study; (ii) received training and follow-up support from a RGPC consultant ; and (iii) inclusion of patients who were willing to discontinue ICS and participate in the study. There was no control group or blinding in this study. One GP per practice gave written consent for practice participation in the study. Patients received study information and gave written informed consent before de-identified information on their ICS withdrawal attempt was forwarded to the project team.
Data collectionParticipating practices kept a registration list of patients that stopped ICS use. This list included some characteristics of the patients (gender, age, smoking status), inhaler medication used before and after ICS withdrawal, occurrence of moderate to severe exacerbations in the 3 months after ICS withdrawal (defined as hospitalizations, antibiotics use, and/or prednisone use), and restarts (if any) of ICS including the reasons (e.g., newly diagnosed asthma). Patients that did not want to participate in the study but did agree to quit ICS were reported without further details on their characteristics or the success of their ICS withdrawal attempt. Participating patients were asked to fill out an online questionnaire after three months on their experience and satisfaction with ICS withdrawal.
Implementation outcomes and safetyAdoption of DECIDE was defined as the number and proportion of practices participating in the COPD IDM program with the intent to actively reduce inappropriate ICS use in their COPD patients. Fidelity was assessed across three key aspects:
ICS withdrawal – To ascertain the extent to which ICS was discontinued in COPD patients who do not benefit from it, assuming that 25% of the COPD population had a valid ICS indication8.
Respiratory medication management after withdrawal – This evaluated whether post-discontinuation prescriptions followed guideline recommendations, specifically whether a long-acting beta-2 agonist (LABA) and/or long-acting muscarinic antagonist (LAMA) was prescribed30. The Dutch guideline for general practitioners recommends to prescribe either a LABA or a LAMA, with no specific preference for LAMA.
Justification for restarting ICS – Was ICS reintroduced for a clinically appropriate reason (i.e., a new asthma diagnosis), or due to a moderate to severe exacerbation.
Safety was operationalized as the number of moderate and severe exacerbations after ICS withdrawal.
Part 3. Semi-structured interviews in patients and practice nursesInterviews based on grounded theory methodology were used to explore patients’ and PNs’ experiences and attitudes towards the DECIDE strategy31. Patients with COPD and PNs that participated in the prospective study (Part 2) were approached for semi-structured interviews. All PNs who volunteered to be interviewed were practice nurses that supervised patients with COPD in their ICS quit attempts.
The interviews took place between September 2022 and May 2023 by two experienced interviewers (IM, LB). The interview guides were used flexibly and were modified to accommodate new topics identified by participants. An online communication platform (Zoom) was used to interview participants by video or audio only, depending on the interviewee’s preference. The interviews for patients lasted between 15 and 30 min, for PNs 20–45 min. The interviews were summarized by the interviewer and three randomly selected summaries of patient and PN interviews were checked for accuracy against the recordings by the second interviewer.
AnalysesCharacteristics of the COPD patient population in Drenthe were described in numbers with percentages. General practice characteristics were described in medians with 25–75 percentiles (unless stated otherwise). For Part 1 change in the percentage of patients with ‘current ICS use’ (from Q1 2022 to Q2 2023: 6 time points of measurement) was estimated using a beta regression model that included time (i.e., Q1-2022 to Q2-2023), general practice category (i.e., category A, B, or C) and time * general practice category interaction terms with the passive exposure group (group C) as reference category. Statistical significance was set at p < 0.05, with p < 0.01 considered highly significant.
Statistical analyses were performed using SPSS version 27.0 (IBM) and betareg package in R (version 2025.05.0). Atlas.ti version 23 (ATLAS.ti Scientific Software Development GmbH) was used to code and analyse the patient and PN interviews. Open coding was used followed by axial coding and finally selective coding. Coding was done by two authors (LB, JG). After the coding of the first three interviews, the two evaluators compared and aligned their coding to ensure consistency.
Comments (0)