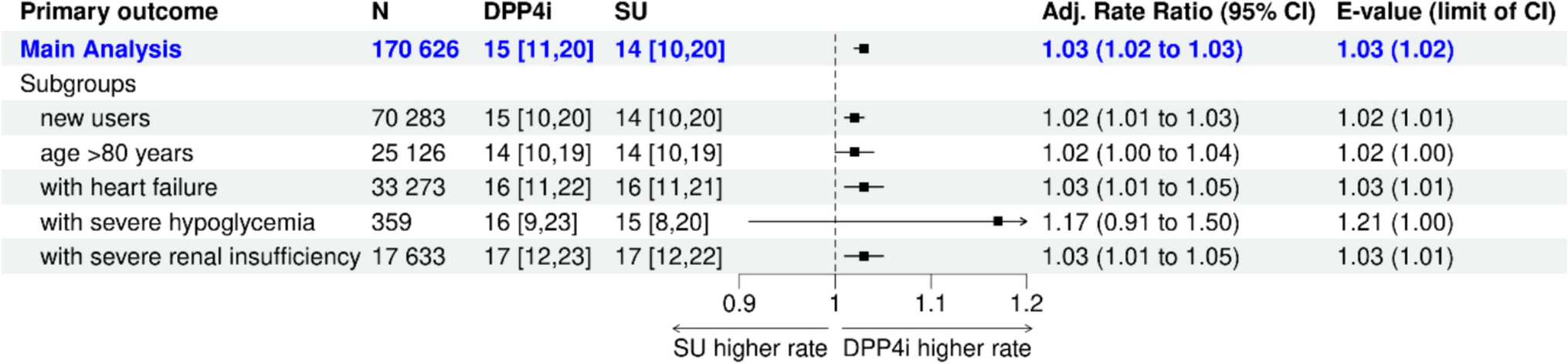
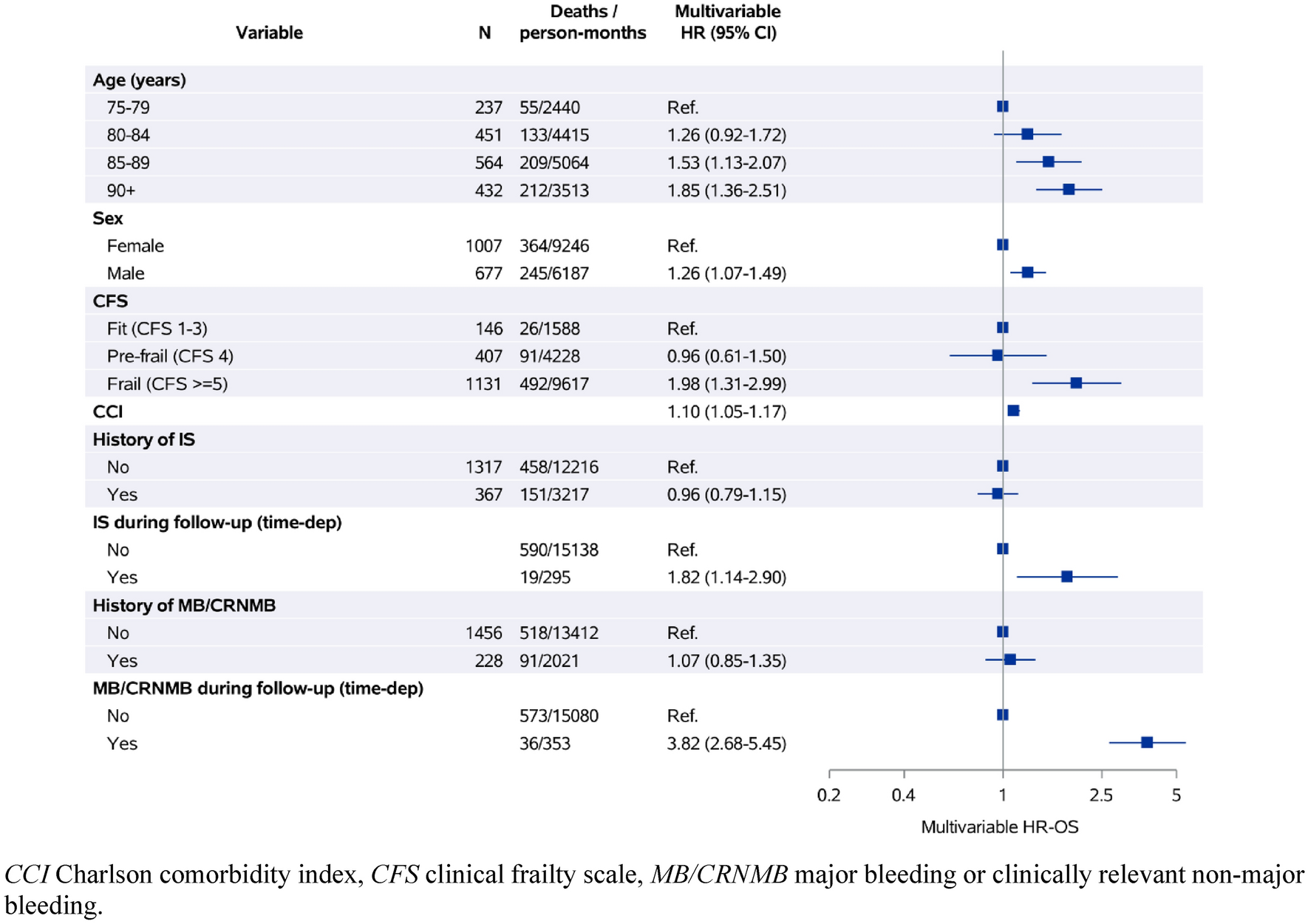
Key Results In this large cohort study based on claims data, the rate of hospitalizations and physician visits within 1 year was slightly higher in DPP4i users compared with patients who received sulfonylurea, but the effect is subject to risk of bias due to unobserved confounding and was very small. There were robust results for a harmful effect of sulfonylurea on the odds for severe hypoglycemia in the subgroups of new users and patients with severe renal insufficiency. This confirms the existing convincing evidence that sulfonylureas cause hypoglycemia in frail older adults.
Limitations We used the concept of target trial emulation, which helps to avoid design-inflicted biases such as selection bias and immortal time bias. Nevertheless, an analysis of sources of remaining bias is always indicated, as even carefully designed analyses sometimes may produce implausible results [24].
Our systematic approach for identifying the relevant confounders can be considered a strength of the analysis. Nevertheless, we identified two sources of potentially important confounding bias that we could not fully adjust for in the analyses. These are physician preferences and the patients’ history of diabetes treatment. The observation that prescribing behavior differs by the number of patients a physician was treating throughout the study (Online Resource 2 Supplementary Table S2) suggests that the treatment decision might often depend on the specialization, experience, or personal preference of the treating physician rather than patient characteristics. The results for the primary outcome have a particularly high risk of being affected, as provider contacts might be strongly influenced by both the treating physician and the treatment history. The latter relates in particular to confounding by indication of switching, which in this case might occur if patients switch the treatment owing to unspecific symptoms that continue to cause increased provider contacts after switching without actually being associated with the treatment. This strong unobserved confounding, combined with the low E-values in the total population and even lower values in the subgroup analyses, suggests that the already low effect size for the primary outcome might be additionally inflated to the null. Further, as our confounder selection was based on the judgment of a single pharmacological expert, it is possible that we missed factors that influence treatment choice for other physicians. However, our approach combined expert judgment with a literature review, which should have minimized the likelihood of missing influential confounders.
Another limitation of the study is the potential for misclassification and missing data in the definition of treatment, confounders, and outcomes. The completeness of diagnoses in the used claims data varies strongly by indication and decreases with age, as a recent comparison of BARMER claims data with survey data shows [25]. Diabetes diagnoses appear to be reliably reported, while for adiposity, myocardial infarction, hypertension, coronary artery disease, and heart failure, between 3 and 15% of self-reported diagnoses are not captured in the claims data for patients over 65 years old. We only considered severe hypoglycemia because only this is coded in ICD-10, but less severe events that do not require hospitalization rely on patient reports and are thus not reliably reported. Of note, even severe hypoglycemia may be under-documented as such cases are often not coded correctly as the primary diagnosis in German hospitals [26]. In addition, our primary outcome may be underestimated as ambulatory cases in Germany are primarily reimbursed through quarterly flat-rate payments, which can include multiple visits within the quarter. This might distort the effect size, but owing to the active comparator design, the directions of effects should not be affected.
One further source of influence on the number of hypoglycemic events is the fact that DPP4i patients more often initiated insulin in the 2 years before baseline (20.2%) compared with sulfonylurea (13.1%; Online Resource 2 Supplementary Table S3). Insulin treatment, irrespective of concomitant antidiabetic drugs, increases the odds for hypoglycemia and may account for the apparently high risk of DPP4i patients for this type of adverse event [9]. The relatively high rate of insulin co-prescription indicates a more intensive blood glucose-lowering strategy associated with a higher risk for hypoglycemia. Furthermore, our analysis did not account for potential differences in co-medications and adherence between groups during follow-up, which could have influenced the outcomes. We estimated the intention-to-treat effect, which reflects the effect of a one-time intervention on the treatment decision, irrespective of later changes to the treatment. Given the limitations of claims data, estimating a real per-protocol effect, for example, only considering adherent patients, is not possible, as we lack information on whether patients take their medications as prescribed.
Interpretation A previous systematic review and meta-analysis by Doni, Bühn [10] did not reveal a difference in the overall risk for adverse events between DPP4i and sulfonylurea as add-on to standard care in older patients. The meta-analyses indicated that DPP4i might decrease mortality, but the estimated effects were not precise. There is more certain evidence for a harmful effect of sulfonylurea on the risk of hypoglycemia. However, the magnitude of the effect is unclear as there was large heterogeneity between studies [10].
A recent subgroup analysis of the CAROLINA trial bolstered these findings in favor of DPP4i and additionally suggested a decreased risk for falls or fractures and cardiovascular events compared with sulfonylurea across all age groups [2]. Previous observational studies found a harmful effect of sulfonylurea on hypoglycemia in older incident users [11,12,13,14,15,16,17], but in agreement with our findings, no difference in mortality between the two drugs [13, 17, 18]. To our knowledge, no previous real-world evidence on the comparison of DPP4i and sulfonylurea exists for overall adverse events and hospitalizations in older adults.
The findings of this study provide insights into the variation in side effects between specific subgroups of older patients. New users and those with severely decreased renal function might have a higher risk for hypoglycemia under sulfonylurea when compared with DPP4i. In contrast, in the population including SU-experienced users, the risk for severe hypoglycemia appears not to be higher than under a DPP4i. The explanation may be that physicians and patients decide to continue sulfonylureas as long as no adverse events occur. Well-informed patients can adapt their diet and react to symptoms of hypoglycemia to prevent severe adverse events. However, in frail older patients, sulfonylureas are not the first choice.
These findings indicate that deprescribing of sulfonylureas and using DPP4i instead may avoid some harms at least in specific subgroups of elderly people and, thus, support existing PIM lists, including the AGS Beers criteria, the PRISCUS 2.0 list, and FORTA criteria. On those lists, sulfonylureas are described as “should be avoided in older adults,” and DPP4i are generally considered safer alternatives.
The observation that some physicians apparently prefer one specific drug over others, more concretely prescribe either only sulfonylureas or DPP4i, suggests a neglect of individualized therapy. The findings thus confirm previous studies that indicate resistant prescribing habits [27].

Comments (0)