
Remember me







The study was a single-centre and one-group pretest‒posttest design clinical trial approved by the Reproductive Medicine Ethics Committee of Xiangtan Central Hospital in March 2018 (s20180322), and registered in the Chinese Clinical Trial Registry (registration number: CHICTR1800016769). The inclusion criteria for this study were a history of infertility due to IUA or multiple failed transplants; age 20–40 years; recurrent moderate-to-severe IUA by hysteroscopy; normal liver, heart and kidney function; no infectious diseases such as HIV, hepatitis B or C, or syphilis; and reproductive intent. The degree of IUA was assessed in accordance with the American Fertility Society (AFS) (1998) scoring criteria. The exclusion criteria were chromosomal karyotype abnormalities, adenomyosis of the uterus, a history of malignant tumour, the presence of a serious physical disease, surgical site infection, coagulation dysfunction, and severe mental or psychological illness. Each participant was informed of the content of the study and signed an informed consent form. The work has been reported in line with the STROCSS criteria [22]. A total of 15 eligible patients with recurrent moderate to severe IUA (AFS score ≥ 6) were recruited between 2018 and 2020, and their clinical characteristics were summarized in Table 1.
Table 1 Patients information and clinical dataIsolation and culture of endometrial stem cells from human endometrial tissuesEndometrial tissue was acquired by hysteroscopy three to seven days after menstruation. The IUA patient was placed in the lithotomy position, the adhesion in the uterine cavity was mechanically separated under hysteroscopic observation to restore the uterine anatomy structure, and the IUD was applied after surgery. A small amount of endometrial tissue was obtained and sent to the laboratory for endometrial stem cell culture during the operation. Then, in a sterile environment, the endometrial tissue was immediately washed 5 times with phosphate buffer saline (PBS) buffer containing 100 IU/mL penicillin and streptomycin to remove blood stains and cut to a diameter of < 1 mm. Subsequently, 0.1% type I collagenase (approximately 3 times the volume of the tissue) was added to the sample, and the sample was mixed and oscillated on a constant-temperature shaking table at 37℃ for digestion for 60 min. DMEM/F12 medium containing 10% Fetal Bovine Serum (FBS) was added to terminate the digestion. After blowing the cell suspension, the suspension was filtered through a screen (40-µm aperture), and the filtrate was the stem cell suspension. Then the mixture was centrifuged at 1500 r/min for 5 min, the supernatant was discarded, an appropriate amount of PBS was added, the mixture was resuspended, the mixture was centrifuged again, the supernatant was discarded, DMEM/F12 medium containing 10% FBS was added for resuspension, and the mixture was cultured at 37℃ in a 5% CO2 incubator. After 24 h, the culture medium was changed every 2 days, cell morphology and cell growth were observed with an inverted microscope every day, and images of the cells were obtained. When the degree of cell fusion reached approximately 90%, cell passage was performed.
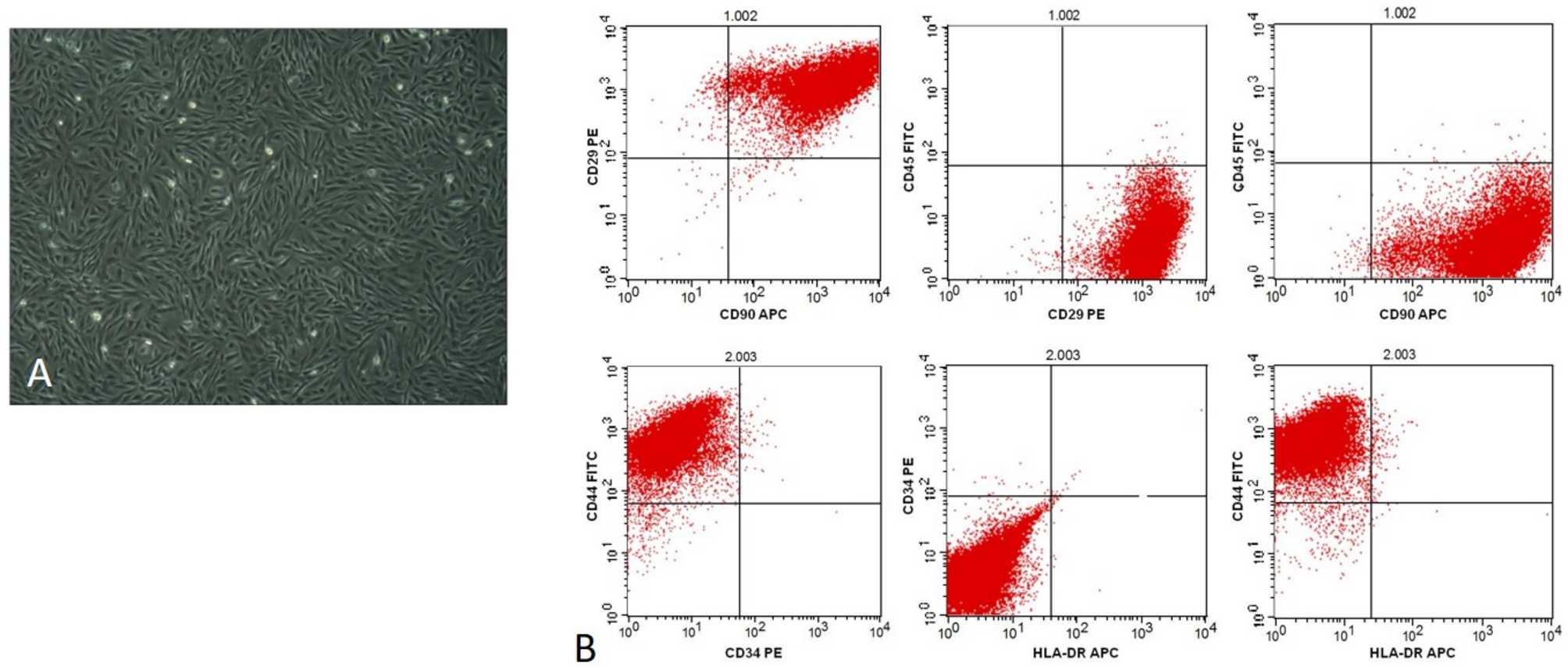
After isolation and culture from endometrial tissue, the endometrial stem cells exhibited a strong proliferation ability, their morphology was uniform with long spindles, and they grew in a whirlpool shape when growing to the fusion state, reflecting the typical characteristics of clonal growth (Fig. 1A).
Fig. 1
Identification of endometrial stem cells. (A) The morphology of endometrial stem cells under microscope. (B) The phenotype identification of second generation endometrial stem cells by Flow cytometry
Cell identification (flow cytometry)Second-generation endometrial stem cells with 90% confluence were digested with 0.25% trypsin-EDTA and prepared as single-cell suspensions. The suspension was centrifuged at 1500 r/min for 5 min, and the supernatant was discarded. The corresponding antibody working solutions (FITC-CD45, FITC-CD44, PE-CD29, PE-CD34, APC-CD90 and APC-HLA-DR) were added, and the negative controls were FITC-IgG1k, PE-IgG1k and APC-IgG1k, respectively. The mixture was subsequently centrifuged at 1500 r/min for 5 min, the supernatant was discarded, and 0.5 ml of PBS was added for resuspension. Flow cytometry revealed that common stem cell-positive (CD29, CD44, and CD90) and negative (CD34, CD45, and HLA-DR) surface markers were identified in second-generation endometrial stem cells (Fig. 1B).
Selection of the sodium hyaluronate gel concentrationSince the stem cells did not reach the ovary immediately after being injected into the uterine cavity, sodium hyaluronate gel was injected to increase its residence time to avoid loss. To avoid the interference of sodium hyaluronate gel on stem cell growth, a CCK8 assay was used to measure the proliferation of endometrial stem cells in sodium hyaluronate gel at different concentrations.
The endometrial stem cells were inoculated into 96-well plates at a concentration of 1 × 104 per well and cultured with a mixture of sodium hyaluronate gel (12.5%, 25% and 37.5%) and complete medium after 2 h of cell adhesion. Then 10 µL of CCK8 detection solution was added at 24, 48 and 72 h. After incubation at 37℃ and 5% CO2 for 2 h, the absorbance in each well was measured at a wavelength of 450 nm. As the proportion of sodium hyaluronate gel increased, the proliferation rate of the endometrial stem cells was slowed and 12.5% sodium hyaluronate gel was determined to be the best choice (Fig. 2).
Fig. 2
The proliferation of endometrial stem cells with different concentrations of sodium hyaluronate gel(*P<0.05)
Transplantation of endometrial stem cellsEndometrial stem cell transplantation was performed on the first day after menstruation. A total of 1 × 107 fifth-generation endometrial stem cells were resuspended in 1 ml of autologous plasma and taken to the operating room for intrauterine infusion. The stem cells were infused by means of a 1 ml injector, and then 2 ml of 12.5% sodium hyaluronate gel was poured into the uterine cavity. After lying down and resting for 30 min, the patient got out of bed and performed some activities. At the same time, the patient was given Oestradiol valerate tablets (3 mg/ day) and acetylsalicylic acid (50 mg/ day) for endometrial support.
Follow-upAfter stem cell transplantation, menstruation in patients was recorded regularly every month. The degree of IUA and endometrial thickness (10–16 days after menstruation) were monitored by hysteroscopy and ultrasonography during the second month after stem cell transplantation; if the endometrial thickness was not greater than 6 mm, a second round of autologous endometrial stem cell transplantation was performed. Monitoring by means of hysteroscopy and ultrasonography was subsequently performed every 2–3 months. When the uterine adhesions were significantly relieved, 2–3 Grade I embryos were thawed and transplanted with the patient’s consent. After transplantation, the patient was given hormonal support consisting of progesterone (600 mg/ day) and oestradiol (6 mg/ day). The concentration of human chorionic gonadotropin (HCG) in peripheral blood was measured 14 days after embryo transplantation to determine whether the pregnancy was successful. Pregnancy status was then followed up by telephone every 3 months until the end of pregnancy, and all patients were followed up until May 2021.
RNA sequencingPrimary endometrial stem cells from 4 healthy individuals (G0), the primary generation of endometrial stem cells from 7 IUA patients (IUA-G0), and the fifth generation of endometrial stem cells from 6 IUA patients (IUA-G5) were used for RNA sequencing analysis. Once the number of cells met the requirements, standard RNA-seq procedures were initiated, including reverse transcription into cDNA, adapter ligation, amplification, and sequencing, were initiated to obtain the raw data.
Screening of differentially expressed genes (DEGs) and functional enrichment analysisAfter quality control of the raw data, the DEGs of IUA-G0/G0 and IUA-G5/IUA-G0 were analysed with Deseq2 software. The screening conditions were p values < 0.05 and| log2(fold change)| > 1. Gene Ontology (GO) and Kyoto Encyclopedia of Genes and Genomes (KEGG) enrichment analyses were performed with R-package clusterProfiler. The GO analysis included cellular component (CC), molecular function (MF), and biological process (BP).
Statistical analysisAll the data in this study were analysed with SPSS 18.0 software and the R software (version 4.3.3). The differences in endometrial thickness and AFS score before and after endometrial stem cell treatment were analysed by means of paired t-test, and P < 0.05 was considered to indicate a significant difference.
Comments (0)