
Remember me
Intensive care of newborn infants relies on adequate monitoring of respiration, circulation, nutrition, and fluid status. This requires, at least during the initial 1–2 postnatal weeks, the use of indwelling catheters for hemodynamic monitoring and repeated blood sampling for monitoring of blood gasses and electrolytes. Such samplings are initially frequent (often several times daily) and require, depending on laboratory method, blood volumes in the range of 0.2 (point-of care analyses) to 1–2 ml (blood cultures), often amounting to a total phlebotomy loss of 10 ml in the first 1–3 days [3], sometimes more (Table 1). Assuming a blood volume of approximately 80 ml/kg, lab draws of 10 ml in the first few days are considered negligible in the term infant ( ~ 3.5% of the blood volume of a 3600-g infant). However, 10 ml corresponds to ~10% of blood volume in a 1200-g newborn. In a 400-g infant, 10 ml of blood draws make up nearly a third of blood volume, and infants this small may have a phlebotomy loss corresponding to their entire blood volume within only a few weeks [3]. Notably, when an institutional protocol for lab draws after admission requiring 10 ml is designed to cover all extremely preterm or extremely low birth weight infants, this means that a 900-g 26-week infant will have ~14% of blood volume removed, whereas a 400-g 22-week infant will have ~31% of blood volume removed. This difference in phlebotomy loss is the equivalent of multiple blood transfusions.
Table 1 Typical blood draw volumes.Volume effects of maintaining line patencyCentral venous lines and arterial lines, including peripheral arterial lines, peripherally-inserted central catheters, and umbilical venous and arterial catheters, require fixed-rate infusions to maintain line patency. Likewise, flushes are frequently used following blood draws and with administration of medications. Due to the same “tiny baby math” effects described above, both the volume and composition of line patency fluids and flushes have a disproportionate impact on small babies.
A common fluid volume rate used for line patency is ~ 0.5 ml/h. Flush volumes are typically 0.3 ml (medications) to 1 ml (blood sampling from indwelling catheter). For a baby with 10 lab draws (Table 1) from an umbilical arterial catheter (UAC) and medications given during the first days, this would amount to flush volumes of 6–8 ml per 24 h. With a line patency rate of 0.5 ml/h, this gives 12 ml of volume daily. For the term infant above, the flushes contribute ~2 ml/kg/d and UAC ~ 3 ml/kg/d, totaling ~5 ml/kg/d. However, for a 1200 g baby, the same flush and line patency strategy would require ~15 ml/kg/d; for the 900 g baby, 20 ml/kg/d; and for the 400 g baby, 45 ml/kg/d. Although line patency fluids and flushes might be considered “negligible” for a term baby, a very low birth weight baby, and even a larger extremely low birth weight baby, this is not the case for a 400 g baby, for whom line patency fluids and flushes, at 45 ml/kg/d, contribute substantially to total fluid intake. In a 400 g baby with a total fluid allowance of 100 ml/kg/d on the first postnatal day (as might be appropriate in some hospital’s conditions if there is little transepidermal water loss—for example, due to very high incubator humidity), nearly half of the fluid intake may be from non-nutritive parenteral fluids [4].
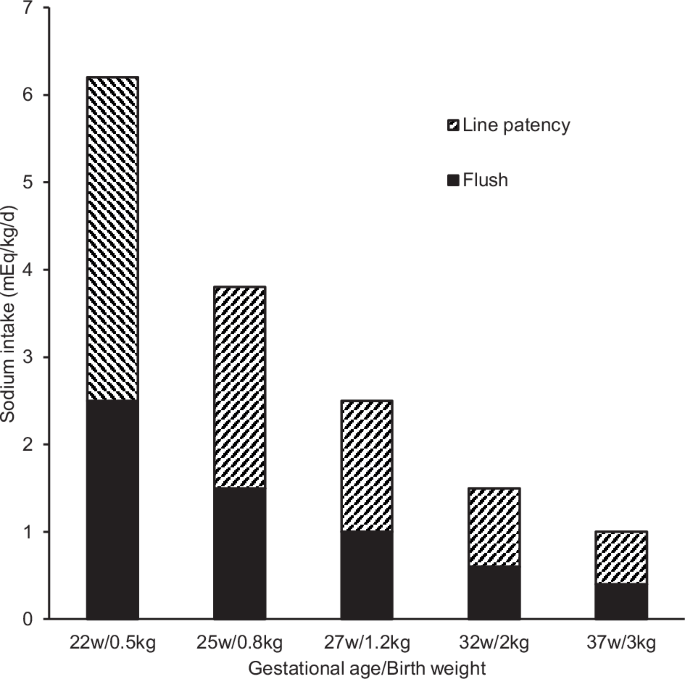
Sodium burden related to maintaining line patencyA sample calculation of the daily sodium load received from a commonly used standard line patency infusion at 0.5 mL/h combined with a daily flush total volume of 8 ml, both with normal saline (NS), is given in Fig. 1. For a 3600 g baby, line patency fluids might give 0.5 mEq/kg/d of sodium, whereas for the 400 g baby, they would provide 4.6 mEq/kg/d. This amount of sodium is easily more than would typically be provided in parenteral nutrition during the first postnatal days. Considering a urine output of 90 ml/kg/d [4, 5] with urine sodium concentration of 80 mM [6] and desired initial daily loss of extracellular fluid (body weight) of 3% (30 ml/kg/d with [Na] = 145 mM [7]), the maximum initial sodium allowance can be estimated as approximately 3 mEq/kg/d [4, 7]. Due to the effects of “tiny baby math,” sodium administration from otherwise negligible sources can easily become too high in the smallest infants [8,9,10].
Fig. 1
Sodium load with line patency fluid of normal saline at 0.5 ml/h + flushes of 8 ml.
Line heparinizationWhile not universally practiced, heparin is often added to intravenous solutions at varying concentrations (0.25–1 U/ml), and has been shown to prolong the duration of line patency [11]. Although this practice has not been evaluated in the most immature infants, both the concentration and rate of infusion of heparin together with infant size are subject to “tiny baby math” considerations. A heparin-containing fluid of 0.5 U/ml running at a rate of 0.5 ml/h in an umbilical artery catheter of a 3600 g infant imply a heparin dose of ~2 U/kg/d while a similar infusion in a 400 g baby gives 15 U/kg/d. Given that neither the clearance nor the pharmacodynamic properties of heparin have been studied in these vulnerable patients, it seems prudent to use the lowest effective dose and to limit the use to infusions running at a low rate.
Endotracheal tube and mechanical ventilationIn the smallest infants, tracheal length (distance from cricoid to carina, has been estimated to be 20–22 mm [12]. The mid-tracheal level (corresponding to the body of the T1 vertebra) is considered optimal for endotracheal tube (ETT) tip placement, and the tolerance for variation in position is related to the length of the trachea. Although the widely known Tochen method [13] for ETT placement in neonates (Depth in cm = 6 + Weight in kg) has been complemented by more recent recommendations [14,15,16] for infants below 1000 g, placement of ETTs too deep is common in EPT infants. Centers in the US, Europe, and Japan within the Tiny Baby Collaborative, all with decades of experience of actively treating infants born at 22–23 weeks, initially place the ETTs at ~5.5 cm. This depth should be appropriate (although borderline) also in infants as small as 400 g. Further, in these centers the use of 2.0 mm internal diameter ETTs is commonplace [17, 18], irrespective of mode of ventilation.
There are several other aspects of respiratory care that are likely to be disproportionally affected by small infant size. Apart from the immaturity-related differences in lung structure, infants at these gestations have a relatively greater anatomical dead space [19] and are mechanically ventilated with tidal volumes that are several orders of magnitude smaller than the ventilator circuit. Irrespective of the mode of ventilation applied, there exist important technical questions about how such small volumes are adequately sensed and compensated for by the ventilator software, and the impacts on respiratory management and outcomes.
Comments (0)