
Remember me
This was a superiority cross-over randomised controlled trial performed in the neonatal intensive care unit (NICU) of a tertiary neonatal unit. It included premature infants who were a minimum of 28 weeks corrected gestational age (cGA), at least 600 g at the time of enrolment and who would have been receiving KMC as part of their routine care. We enrolled infants over a five-month period between May and September 2022.
Ethics approval and consent to participateThis study was approved by the Clinical Research Ethics Committee of the Cork Teaching Hospitals, Cork, Ireland. Informed consent was obtained from all the parents prior to randomisation and participation in the trial. Infants with any known neurological abnormalities (other than intraventricular haemorrhage), orthopaedic conditions and/or chromosomal abnormalities were excluded.
Sample sizeAn a priori sample size calculation indicated that a sample of 20 patients was necessary to detect a difference of 2% in NIRS percentage in a cross-over study using a paired t-test comparing 30° and 60° angle positions. This sample size was based on assuming a correlation of 0.5 between paired measurements, a standard deviation of difference of 3, a power of 80%, a level of significance of 0.05 and a 2-tailed test. The sample size calculation was performed using the G-Power 3.1 programme [12].
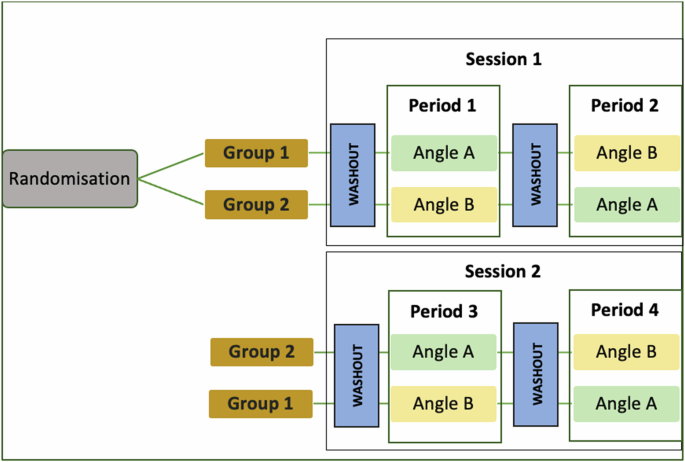
Randomisation and proceduresEligible infants were enrolled by study investigators (IS, SM and SV) and randomly assigned (1:1) to one of two groups. In Group 1, infants began Session 1 at the 30° angle, followed by 60°, and Session 2 at 60°, followed by 30°. In Group 2, infants began Session 1 at the 60° angle, followed by 30°, and Session 2 at 30°, followed by 60° (see Fig. 1). Numbers were generated using a sequence generator, printed out, and stored in sealed, opaque envelopes. When an infant was enrolled, an envelope was selected. If the number inside the envelope was odd, the infant was assigned to Group 1; if the number was even, the infant was assigned to Group 2, as illustrated in Fig. 2. For each session, during routine kangaroo mother care, the NIRS probe was applied to the baby’s forehead and the baby was subsequently placed prone on the parent’s chest. The chair was then put at the starting angle to which they had been randomised and the cerebral NIRS values, heart rate and peripheral saturations were recorded for 30 minutes. The chair was then gently repositioned into the other angle and the baby was observed and the values recorded for a further 30 minutes.
Fig. 1
Randomisation process, timing of sessions and wash-out periods, and measurement periods.
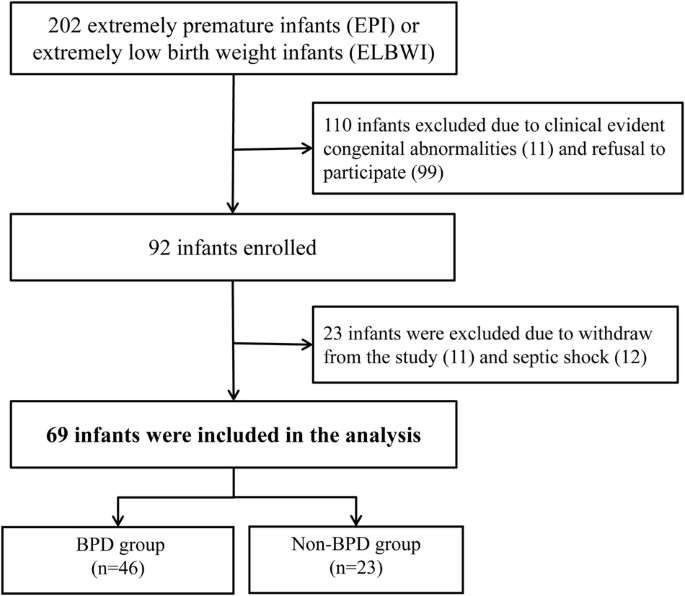
Fig. 2
Consolidated Standards of Reporting Trials (CONSORT) flow diagram of enrolment, allocation to Group 1 or 2 and numbers analysed for the trial.
EquipmentThe chairs used in this study were the Tucson Reclining Mauro Relax Ergo-line medical chair (Haelvoet NV, Ingelmunster, Belgium). These are routinely used in the NICU for the delivery of kangaroo care. This chair can be inclined to 120° at full incline which coincides with the 30° angle used in this study (information on the angles can be found at: https://www.haelvoet.com/en/products/details/354 and illustrated in Supplementary Fig. 1). The 60° angle of inclination was determined using a protractor during the design phase of this study.
Cerebral NIRS was monitored using the Masimo Root with O3 regional Oximetry machine (Masimo, Irvine, California, USA) with the Medtronic INVOS Cerebral Oximetry Infant-Neonatal Sensor (Medtronic Limited, Watford, United Kingdom).
OutcomesThe primary outcomes were cerebral NIRS values during the KMC sessions at both 30° and 60° angles. This consisted of the mean cerebral tissue oxygenation saturation (rSO2) and cerebral fractional tissue oxygen extraction (FTOE) values. The rSO2 is measured as a percentage. The FTOE was calculated using the following formula: (SpO2 − rSO2)/SpO2 [13].
There were four secondary outcomes assessed during the sessions at the two angles: (1) peripheral oxygen saturation (%), (2) heart rate (beats per minute), (3) number of bradycardias <100 beats per minute, and (4) number of desaturations less than 80% lasting longer than 20 seconds.
Statistical analysisCategorical data was described using frequencies and percentages and continuous data using means and standard deviations (SD) (when the data was normally distributed) or as medians and inter-quartile ranges (IQR) otherwise. The effect of the angle (30° or 60°) on the continuous primary and secondary outcomes was investigated using linear mixed effects models with angle as a fixed effect and subject as a random effect. As SpO2 was negatively skewed, bootstrapped 95% confidence intervals (with 10 000 repetitions) were also calculated to assess the sensitivity of the results to non-normality. The conclusions did not change. The effect of the angle on the secondary binary outcomes was investigated using logistic mixed effects models with angle as a fixed effect and subject as a random effect. In the initial models, period and sequence were included as fixed effects to test for period and sequence effects. As there were no significant period or sequence effects, they were removed as fixed effects in the final model. Due to multicollinearity, carry-over effects were not investigated. The four periods were also looked at separately and outcomes compared between the two angles using the Wilcoxon signed rank test. Statistical analysis was performed using IBM SPSS Statistics (version 29.0, IBM Corp., Armonk, NY).
Comments (0)