
Remember me


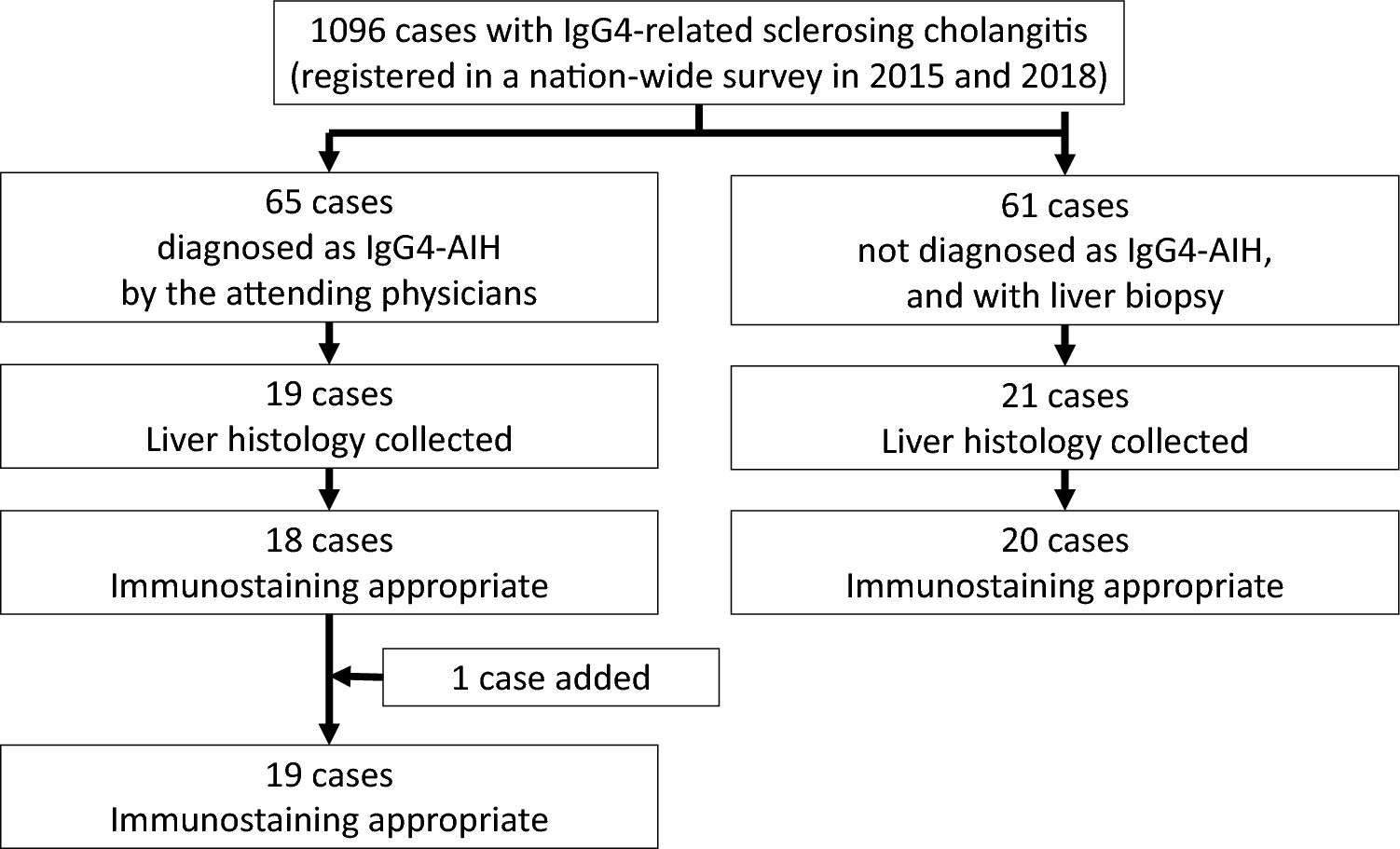
A comprehensive clinical and histopathological analysis of 19 cases of IgG4-AIH, as reported by the attending physicians, revealed that 9 cases were diagnosed as either definite or probable AIH according to the simplified diagnostic criteria. Among the remaining ten cases, two were classified as IgG4-hepatopathy, five as canalicular cholestasis, and three were diagnosed with other diseases; one primary sclerosing cholangitis, and two chronic hepatitis C. In 2 of the 19 cases (AIH-56, AIH-60), IgG4-RD was observed in other organs, suggesting the possibility of IgG4-hepatopathy in the liver tissue.
The histopathological findings of IgG4-AIH in nine cases diagnosed with AIH (AIH-07 to AIH-73) are summarized in Table 1. In three of the nine cases (AIH-07, 12, and 40), IgG4 or IgG immunostaining was either absent or difficult to evaluate, precluding assessment of the IgG4 + /IgG + ratio. In the remaining six cases, three (AIH-14, 29, and 73) met the diagnostic criteria of an IgG4/IgG-positive cell ratio of 40% or greater and 10/HPF or more of IgG4-positive plasma cells. Among these three cases, one case (AIH-29) exhibited a low number of IgG4-positive cells, with an average of 10.1/HPF across three fields of view. These cells were observed only in limited regions of the liver tissue, suggesting a low likelihood of IgG4-AIH in AIH-29. Based on the findings above, only two cases, AIH-14 and AIH-73, met the diagnostic criteria for IgG4-AIH as established in this study.
Table 1 Histopathological assessment of potential IgG4-AIH casesAIH-14 is a previously reported case elsewhere [20]. The patient, a female in her 40 s, presented with elevated aminotransferases levels, along with elevated IgG4 (669 mg/dL), and a positive anti-nuclear antibody titer of 1:160. Histopathological analysis revealed prominent lymphoplasmacytic infiltration accompanied by fibrosis. A notable presence of IgG4-positive plasma cells was observed, with 25.3 cells per high-power field and an IgG4/IgG ratio of 310.2%. Although storiform fibrous and obliterative phlebitis were absent, the patient fulfilled the provisional diagnostic criteria for IgG4-AIH defined in the current study. The histological features were consistent with the acute hepatitis phase of AIH, characterized by diffuse distribution of IgG4-positive cells in the portal areas, lobules, and central lobular regions, with a particularly high concentration in the portal areas. The patient was treated with prednisolone (PSL), leading to a rapid and marked reduction in ALT, IgG, and IgG4 levels. She is currently maintained on 5 mg/day, with no evidence of relapse [20].
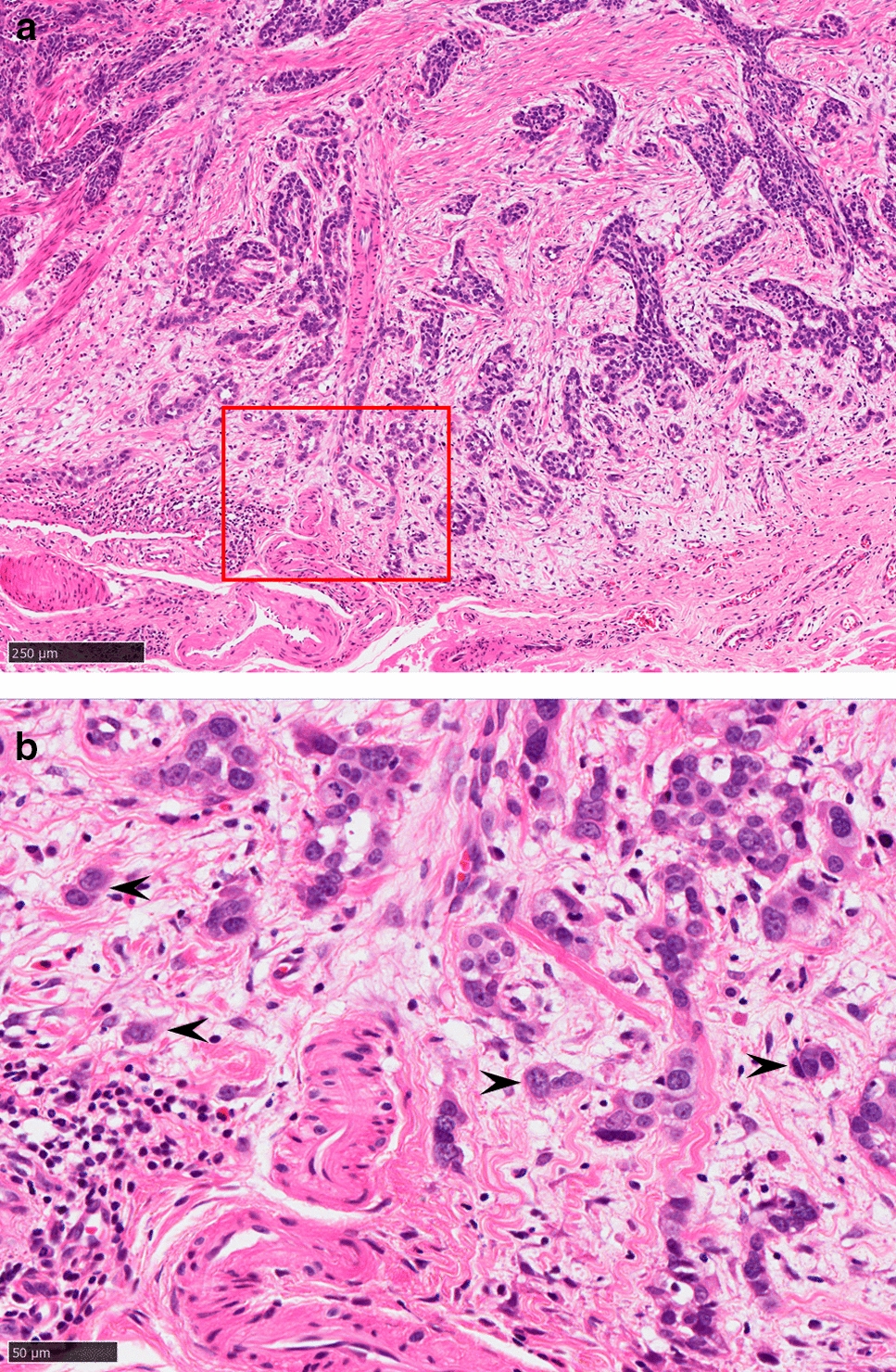
Another case, AIH-73, is a male case in his 50 s, with serum IgG4 of 408 mg/dL. He had IgG4-related sialadenitis and a suspicion of IgG4-SC. Liver biopsy revealed acute hepatitis characteristic of AIH, with significant infiltration of lymphocytes and plasma cells within the portal area (Fig. 2a, b). The numbers of IgG4- and IgG-positive cells were 26 and 29, respectively, in this field (Fig. 2c, d). The findings fulfilled the provisional diagnostic criteria for IgG4-AIH. Notably, there was no evidence of storiform fibrosis or obliterative phlebitis. PSL was highly effective as well and there was no relapse.
Fig. 2
Histopathology of the patient (AIH-73) diagnosed as IgG4-related autoimmune hepatitis (AIH). a, b: Hematoxylin and eosin staining. Panlobular hepatitis with marked lymphoplasmacytic infiltration that is consistent with AIH. c, d: Immunostaining for IgG4 (c) and IgG (d). The numbers of IgG4- and IgG-positive cells were 26 and 29, respectively, in this field
IgG4-hepatopathyA histopathological analysis of IgG4-hepatopathy was conducted in 20 cases where immunohistochemical staining of liver tissue from patients with IgG4-SC was feasible. The findings revealed that six cases (SC-03, 09, 27, 50, 51, and 60) met the criteria for IgG4-hepatopathy, characterized by significant lymphocyte and plasma cell infiltration in the portal area, the presence of more than 10 IgG4-positive cells/HPF, and more than 40% of IgG4 + /IgG4 ratio. In SC-03, where the number of IgG4-positive cells was notably low (10.6/HPF), many plasma cells were crushed during collection, suggesting the actual count may be higher. In addition, two cases (AIH-56, AIH-60), which were diagnosed as IgG4-AIH by the attending physician but did not meet the diagnostic criteria for IgG4-AIH in this study and were instead classified as potential IgG4-hepatopathy, were included.
The results of the histopathological analysis of these three cases are presented in Table 2. Histologically, in addition to lymphocyte and plasma cell infiltration in the portal area, eosinophil infiltration was easily observed in three cases. None of the cases showed evidence of storiform fibrosis or obliterative phlebitis. While some cases exhibited bile duct reactions and cholestasis, the existing intralobular bile ducts were generally preserved, with bile duct abnormalities observed in only one case. Figure 3 presents the liver histopathological findings (HE staining, IgG, and IgG4 staining) from two representative cases (SC-50 and AIH-56) out of the eight analyzed. The portal areas are expanded and exhibit infiltration by lymphocytes and plasma cells, with numerous IgG4-positive cells. A high IgG4 + /IgG + cell ratio is also observed, while the existing interlobular bile ducts remain intact (Fig. 3a; Nakazawa classification Type 2a [21]).
Table 2 Histopathological assessment of potential IgG4-hepatopathy casesFig. 3
Histopathology of the patient diagnosed as IgG4-related hepatopathy. a Hematoxylin and eosin staining. In a typical case (SC-50), marked lymphoplasmacytic infiltration was observed without damaging the interlobular bile ducts (arrow) in the portal area (SC-50). b Hematoxylin and eosin staining. In another case (AIH-56) in which the ductular reaction and cholestasis were prominent, the interlobular bile ducts were damaged. Note the interlobular bile ducts adjacent to the interlobular arteries (arrows) were absent. c, d: Immunostaining for IgG4 (c) and IgG (d) in SC-50. The numbers of IgG4- and IgG-positive cells were 120 and 155, respectively, in this field, which was isomeric with a high-power field
Clinical features of these eight patients are shown in Table 3. Seven out of eight cases were male, and all were over 60 years old. Since all cases were extracted from the nationwide survey of IgG4-SC, all eight cases were complicated by IgG4-SC, with two cases also having concurrent AIP. Among the eight cases with IgG4-SC, two were classified as Type 2, two as Type 3, three as Type 1, and one as Type 4, according to the Nakazawa classification [21]. All cases were treated with immunosuppressive drugs, resulting in favorable therapeutic responses.
Table 3 Clinical features of potential IgG4-hepatopathy cases
Comments (0)