Patients
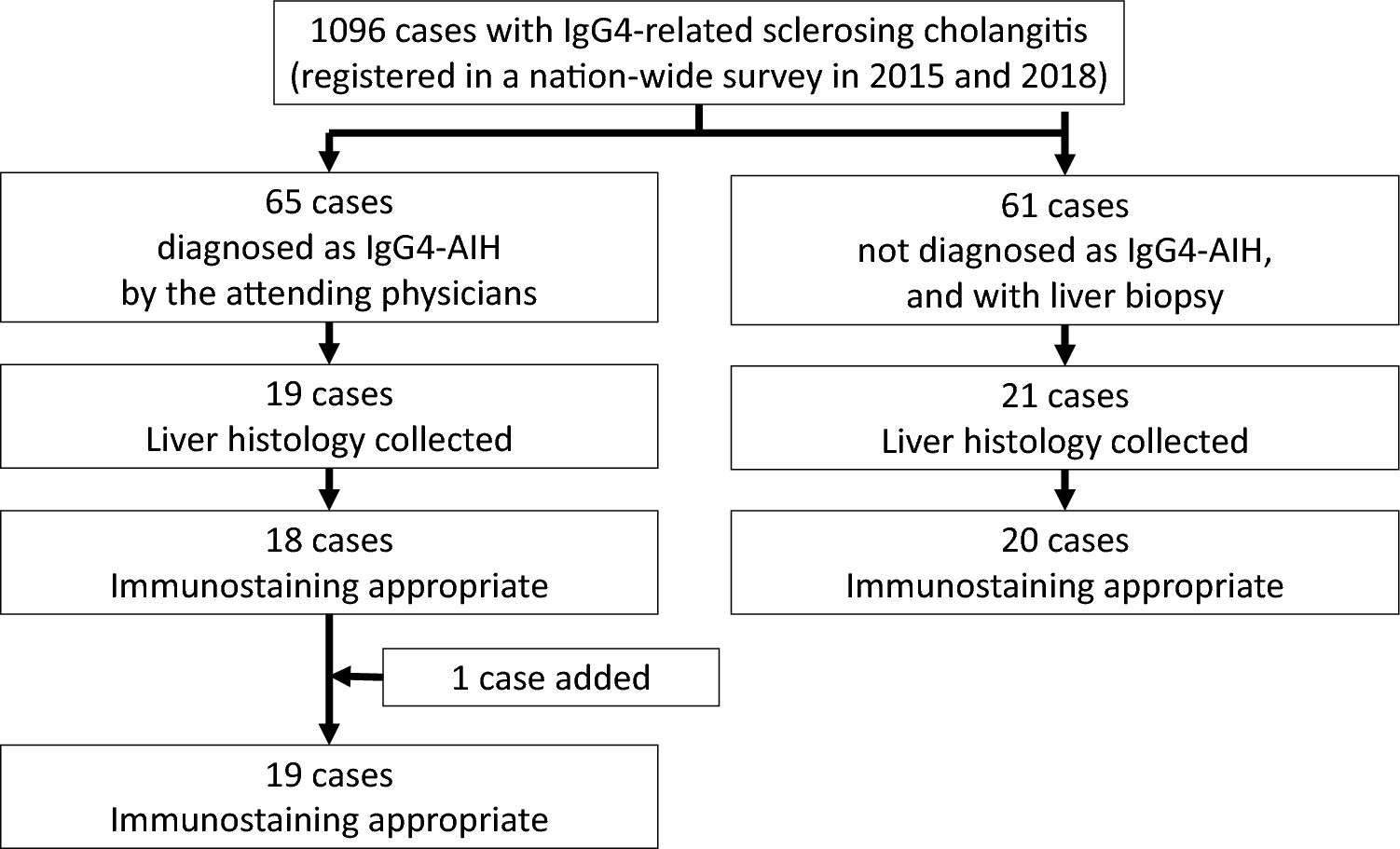
This was a retrospective, multi-center study of CD patients. The inclusion criteria were as follows: (1) diagnosed with CD based on clinical, endoscopic, and histological criteria; (2) with a history of outpatient visits or hospitalization at our hospital and collaborating institutions; (3) age≧18 years; (4) had LRG values measured by Nanopia (Sekisui Medical, Tokyo, Japan); and (5) the ileum can be adequately evaluated via retrograde BAE (EN-580XP, FUJIFILM Corporation, Japan; SIF-Q260, OLYMPUS CORPORATION, Japan) or long-narrow colonoscopy (PCF-H290, OLYMPUS CORPORATION, Japan) including selective contrast examination at the deepest point reachable by the endoscope. Conversely, the exclusion criteria were as follows: (1) having an interval of > 30 days between endoscopy and LRG measurement; (2) treatment modification between endoscopy and LRG measurement; (3) contraindicated for BAE because of severe SB strictures detected radiographically, (4) severe extraintestinal manifestations and anal lesions; and (5) any cancer. No exclusion criteria were established for disease duration, and initial diagnostic CD patients were also included in this study. Notably, it was expected that a limited number of patients would have an interval of less than 30 days between endoscopy and LRG measurement, because of the insurance-related time constraints between the two examinations. At all institutions, CD was diagnosed based on the diagnostic criteria of the Ministry of Health, Labor, and Welfare (i.e., “Research on Intractable Inflammatory Bowel Disorders”). This study protocol was approved by the Ethics Committee at Nagoya University Hospital (2023–0449), and the study was conducted in accordance with the Declaration of Helsinki. This study was conducted retrospectively and we guaranteed participants an opportunity for rejection through information disclosure.
Characteristics and outcome variables
The following demographic data were collected: age, sex, disease duration, history of major intestinal surgery (i.e., intestinal resection or strictureplasty), smoking (i.e., current smoker, previous smoker, or non-smoker), anal disease (i.e., perianal abscess or anal fistula), liver cirrhosis, and complications of other immunological diseases. In addition, medication data for the following drugs were collected: non-steroidal anti-inflammatory drugs, steroids, antiplatelet drugs, immunomodulators, infliximab, adalimumab, vedolizumab, ustekinumab, risankizumab, and upadacitinib. All medication data were related to current medication use; the history of previous medication use was unaccounted for. In addition, various liver diseases may affect LRG values (since the liver produces LRG), but the data regarding this were scarce. Thus, only data on liver cirrhosis were collected.
The following outcome variables were collected: Crohn’s Disease Activity Index (CDAI) score, Patient-Reported Outcome (PRO-2), modified Simple Endoscopic Score for CD (modified SES-CD) [12], presence of fistula, location (L1: ileal, L2: colonic, and L3: ileocolonic), behavior (B1: inflammatory, B2: stricturing, and B3: penetrating), as well as the levels of LRG, C-reactive protein (CRP), FC, albumin (Alb), aspartate aminotransferase (AST), alanine aminotransferase (ALT), and hemoglobin (Hb). For these outcome variables, if data were obtained from the same patient multiple times, only the first dataset was used for analysis. Biomarker data were measured on the same day as LRG. If such data did not exist, biomarker data were measured on the date closest to the date of endoscopy. The standard body weight for CDAI calculation was determined as follows: (height in meters)2 × 22. Only Bristol stool scale 6 or 7 was counted for defecation frequency when calculating CDAI and PRO-2 scores. PRO-2 scores were calculated by simple addition of CDAI-1 and CDAI-2 scores without weighting.
Imaging modalities
This study included patients who underwent retrograde BAE, or whose ileum could be adequately evaluated via long-narrow colonoscopy including selective contrast examination from the deepest point of endoscopic reach. Endoscopic evaluations were performed using the modified SES-CD. The SB was divided into following three segments: jejunum, proximal ileum, and terminal ileum, defined as the portion of the ileum observable by colonoscopy. In addition, considering that the length of the SB is ≤ 600 cm, and that the jejunum and ileum are roughly the same length, the terminal ileum, proximal ileum, and jejunum were defined as the segments ≤ 10 cm, 10–300 cm, and 300–600 cm from the ileocecal valve, respectively [12]. The right colon was defined as the segment including the cecum with the ileocecal valve and the ascending colon until the hepatic flexure. The transverse colon was defined as the segment between the hepatic and splenic flexures. The left colon was defined as the segment including the descending colon and sigmoid colon until the rectosigmoid junction; its continuation until the anal side was defined as the rectum.
For the most severe lesion in each segment, a score of 0–3 was given for the following variables: ulcer size, proportion of ulcerated surface, and proportion of affected surface. Stenosis was not included in the modified SES-CD score because this study focused on the relationship between small bowel mucosal lesion activity and LRG levels. The total score obtained for each segment was summed to obtain the modified SES-CD. Modified SES-CD scores of ≤ 3 and ≤ 1 indicated endoscopic remission and complete ulcer healing, respectively [13]. Many of the institutions participating in this study do not routinely calculate the modified SES-CD score. Therefore, one gastroenterologist at each facility who is an expert of BAE reviewed the endoscopic findings from BAE and calculated the modified SES-CD score, ensuring that patient background and laboratory data were blinded to the person performing the calculation.
Combination of target population and endoscopic activity
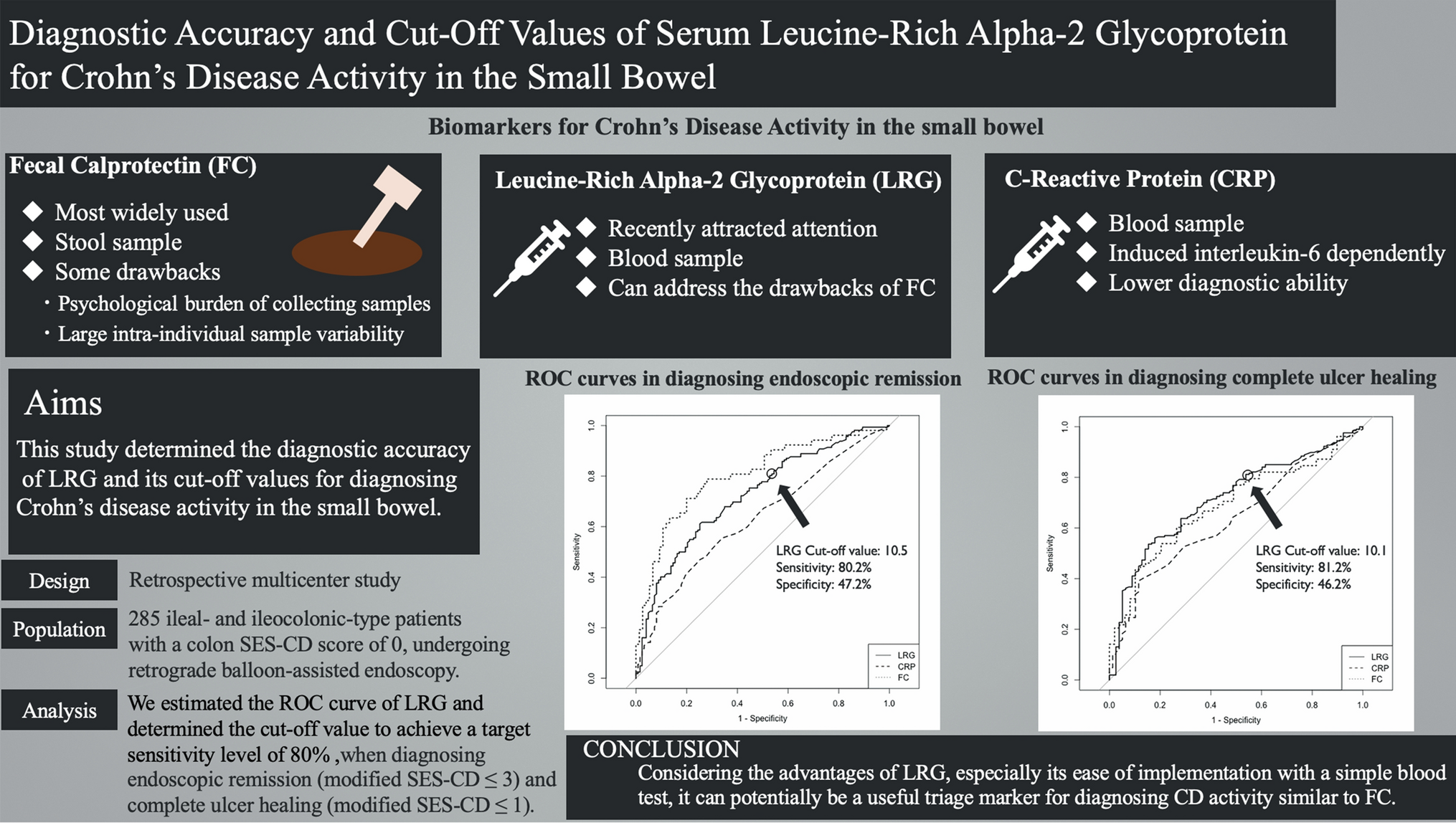
To assess the diagnostic ability of LRG for SB lesions, the target population of SB patients were set as ileal-type and ileocolonic-type patients, both with a colon SES-CD score of 0. In addition, we also set another target population which includes both SB and colon patients, seeing that it would be worthwhile to report the diagnostic ability of LRG in both types of lesions. For all patients, the diagnostic ability of LRG was evaluated based on endoscopic remission and complete ulcer healing.
Statistical analysis
For all combinations of the two target populations (i.e., SB patients alone, SB and colon patients) and two outcome variables of endoscopic activity (i.e., endoscopic remission, complete ulcer healing), the following analyses were conducted. A receiver operating characteristic (ROC) curve of LRG was estimated to evaluate its diagnostic accuracy for CD activity. Since no obvious factor is strongly correlated with CD activity (as confirmed on multivariate logistic regression analysis), the primary analysis involved estimating the ROC curve of LRG without stratification by any factor.
In determining the cut-off values of LRG, we placed an emphasis on sensitivity, because having a high sensitivity minimizes false negatives. This means that a negative LRG result would suggest a high probability of CD inactivity, and thus BAE can be avoided. Conversely, to address the increased false positives, when the LRG is positive, other clinical findings will be considered to determine if BAE should be performed. We targeted a sensitivity of 80% based on previous studies on FC, reporting sensitivities of 82.4% [5] and 75.0% [6]. The ROC curves of CRP and FC were also estimated, and the differences in the area under curve (AUC) between LRG and CRP or FC were evaluated via two-sided Delong’s test. All analyses were performed using R version 4.2.1.



Comments (0)