The present multicenter study, which encompasses 17 health check-up institutes throughout Japan, has successfully demonstrated the sex-related difference in age distribution and risk factors for BE. In particular, we identified a distinctive, paradoxical correlation between two prevalent obesity-related variables and BE, which was exclusively observed in males. Specifically, our findings revealed that a combination of low BMI and high WC was associated with an increased risk of BE in males.
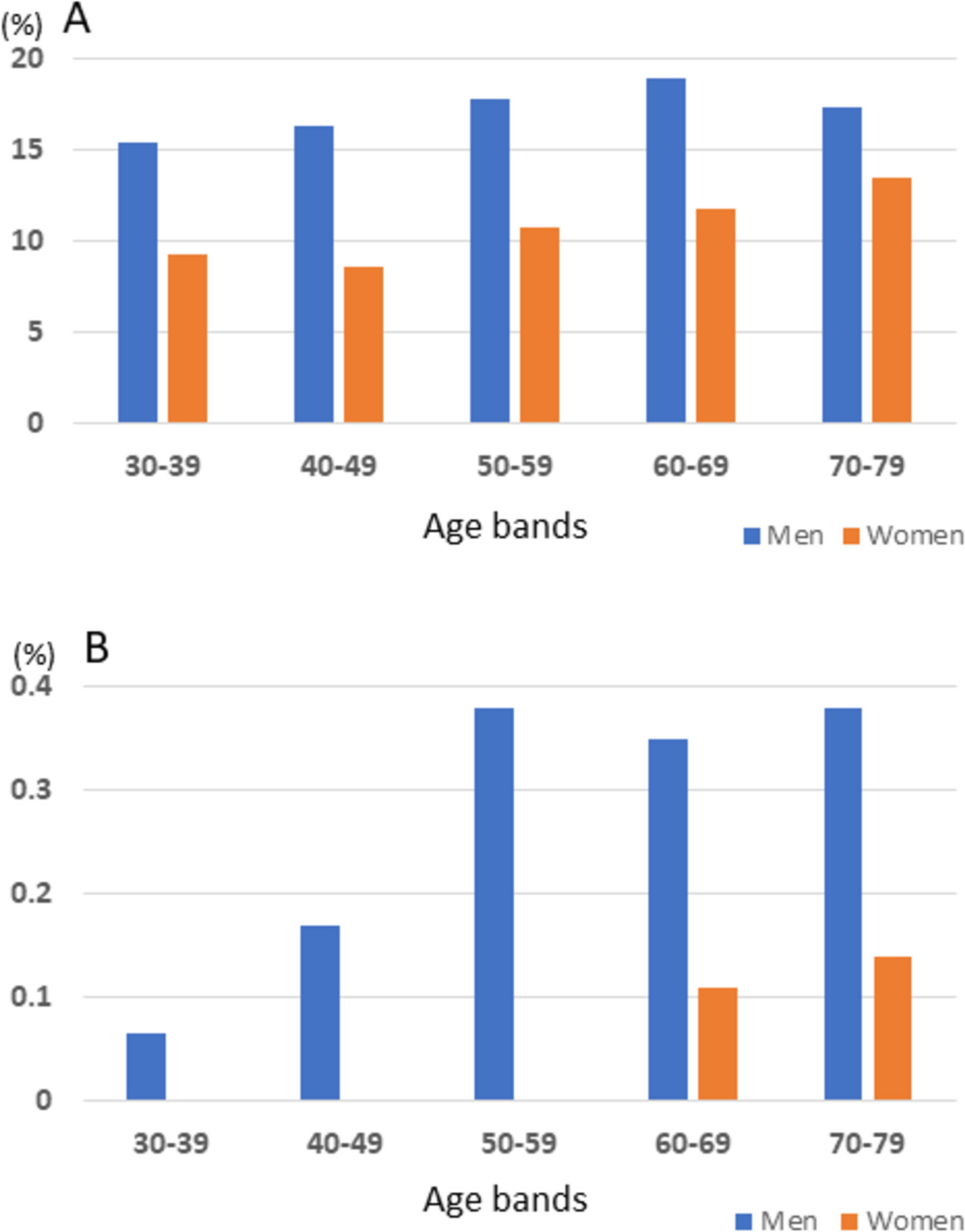
This multicenter study is the first to determine the prevalence of BE by sex within each Japanese age cohort. The overall prevalence of BE is relatively common in both men and women across all age groups in Japanese health check-up settings although it is consistently more prevalent in men than in women. This distribution pattern appears to differ significantly from that observed in Western countries [14, 15], where endoscopic surveillance for BE was introduced in response to a marked increase in EAC [3]. The discrepancy is likely attributable to disparate international diagnostic criteria for BE (e.g., the necessity for histologic confirmation) or distinct target populations (e.g., health screening vs. subjects presenting with heartburn) [11]. Whether this commonly seen BE in Japan should be included in surveillance depends on its carcinogenic potential [8].
Conversely, LSBE is a rare condition, accounting for 0.2% of the entire cohort. Additionally, there are notable discrepancies in the age distribution between men and women. In men, LSBE starts to appear in the 30 s and reaches a plateau in the 50 s, while in women, it is not seen at all until the 50 s and becomes slightly more common in the 60 s–70 s. Thus, the 20- to 30-year time lag observed in the prevalence of LSBE by sex in Japan is consistent with the findings on the entire BE reported from Europe and the United States [14, 15]. Therefore, LSBE diagnosed in Japan, at least, is considered to refer to the same condition as BE diagnosed in Europe and the United States despite different international diagnostic criteria for BE [11]. LSBE has been confirmed to have a high cancer incidence in Japan [16, 17], comparable to that in Europe and the United States, and should be a target for surveillance. Given that BE is known to rarely extend its length throughout life once it appears [18,19,20] and that the prevalence of LSBE in Japanese men reaches a plateau in their 50 s, it may be recommended that periodic endoscopic surveillance be initiated in men at the age of 50. In light of a recent study from the United States that demonstrated an increasing prevalence of BE in the young population, which led to the proposal of an adjustment to the age cut-off to 45 years [21], it is imperative to maintain a continuous and meticulous monitoring of the age distribution of BE in Japan. In contrast, women may be an unlikely target for surveillance as EAC is exceedingly rare [8], and LSBE occurs only slightly at an older age.
Although obesity is a well-recognized risk factor for BE in Western countries [3, 4], it is less clear in Asian countries as a previous meta-analysis showed no significant association between BE and simple obesity represented by BMI in Asians [22]. Several studies in the Japanese population investigated the association between BMI and BE with conflicting outcomes, and few dealt with WC as an indicator of central obesity [23,24,25,26,27]. In the present study, when incorporating BMI and WC in an analytical model together, we found paradoxical associations of the two obesity-related variables with BE, namely BMI is negatively associated with BE while central obesity is positively associated with it. Further, such paradoxical association was observed only in men and is more pronounced in LSBE. Notably, this phenomenon has never been identified in reports on BE in Western countries [28, 29]. Very interestingly, the emerging paradoxical association of BMI and WC with BE in the current study, e.g., low BMI/high WC is associated with BE, seems to coincide with a recent finding from Japan that while BMI is negatively associated with early-stage EAC, abdominal obesity measured by visceral fat area on an abdominal CT image is positively associated with it [30]. Thus, low BMI/high WC seems to be a common risk factor for both BE and EAC in Japanese subjects.
BMI and WC are the two most commonly utilized conventional measures for the diagnosis of obesity. However, BMI is unable to identify adipose tissue and thus is unable to discriminate between fat and fat-free lean mass. Accordingly, the emerging paradoxical association may be explained by the new concept of "sarcopenic obesity," in which the co-existence of obesity and sarcopenia could occur with aging [31, 32]. For example, the loss of muscle mass due to sarcopenia results in a reduction in physical activity and the accumulation of visceral fat. The association between sarcopenic obesity and various age-related diseases, including cancer, has recently attracted considerable interest [31,32,33], and it is noteworthy that Asians are at a greater risk of sarcopenic obesity, including abdominal obesity and low muscle mass, than Caucasians [34, 35]. Therefore, the present study proposes that sarcopenic obesity may be linked to not only EAC but also its precursor BE. This suggests that the identification of candidates for BE surveillance could be further refined by the two easily available obesity-related variables, namely BMI and WC.
Interestingly, RE, regarded as a precursor condition to BE, exhibited a consistent positive association with the two obesity-related variables (See supplemental Table 3). Therefore, the relationship between "obesity" and BE/RE is not uniform. While general obesity is sufficient to increase the risk of developing RE through mechanically induced reflux, sarcopenic obesity is required to increase the risk of BE. Visceral fat, a prominent feature of sarcopenic obesity, is known to be metabolically active and secretes various pro-inflammatory cytokines, such as leptin and adiponectin [4]. These circulating adipokines, released from adipose tissue, may play a crucial role in the pathogenesis of BE [4].
In addition to the obesity-related factors, gastric atrophy is negatively associated with LSBE in this study. Notably, advanced open-type gastric atrophy is identified as a strongly protective factor (e.g., OR = 0.015). This finding is consistent with previous studies in Japan, which have demonstrated that a sufficient amount of gastric acid from a non-atrophic (H. pylori-negative) healthy stomach is a prerequisite for BE, particularly LSBE [36]. In Japan, the prevalence of LSBE is expected to increase in future as the rate of H. pylori infection in the general population declines.
The strength of this study is that the data were collected from multiple screening facilities throughout Japan and is considered to reflect the actual status of screening in Japan. In addition, to begin this study, a consensus meeting was held regarding the diagnosis of BE to unify the diagnosis. In contrast, a dearth of information regarding certain associated factors represents a potential limitation of this study. Consequently, a multivariable regression analysis was conducted on a subset of subjects, resulting in the exclusion of 20.8% of the original sample. However, since these patients' information are basic data systematically collected at screening facilities, the missing data observed in this study can be attributed to difficulties in providing data at each facility, rather than to individual patient characteristics. Further, due to the absence of a standardized response format for smoking and drinking among the participating institutes, this study was only able to categorize these behaviors as either "ever" or "never." Consequently, the results of this study, which demonstrated a negative correlation between these lifestyle habits and BE, should be interpreted with caution.
In conclusion, this nationwide Japanese multicenter study revealed age distribution and risk factors for BE in the Japanese population, stratified by sex. In particular, we found low BMI/high WC is a strong risk factor for BE in the Japanese male population. The findings will provide valuable information for establishing an efficient surveillance strategy for BE in Japan.



Comments (0)