There is growing appreciation for the prominence of non-motor symptoms in patients with movement disorders, including ET. Prospective studies have delineated a diverse range of non-motor features associated with ET, leading to the hypothesis that these symptoms likely antedate the emergence of tremor and thus represent early manifestations of underlying neural pathology rather than secondary responses. Dysfunction within central autonomic pathways may constitute an intrinsic non-motor component of ET with the potential to significantly impair patient quality of life [3].
In an early study by Damian et al., it was concluded that, using the SCOPA-Aut questionnaire, patients with PD showed increased autonomic dysfunction in various domains, while those with ET did not exhibit significant autonomic dysfunction, except for sialorrhea [12]. This study has several limitations. Firstly, it relied solely on a subjective questionnaire, which may not provide comprehensive and objective information about autonomic dysfunction. Secondly, the study did not consider the potential influence of educational, cognitive, and psychiatric manifestations within the studied population. These factors could have a significant impact on their results.
In another study, researchers utilized SSR tests to objectively evaluate autonomic functions in patients with essential tremor ET. The results revealed the presence of sympathetic dysfunction, but no abnormalities were found in the parasympathetic system. However, the exact reason for the lack of parasympathetic dysfunction remains uncertain and could potentially be attributed to technical issues. Overall, the study's findings suggest the presence of sympathetic dysfunction in patients with ET [13].
Building on inconclusive findings from previous studies, we conducted our research to explore the potential presence of autonomic system dysfunction in patients with ET. For our investigation, we compared 30 ET patients with a control group consisting of 30 subjects. Both groups did not show significant differences in terms of gender distribution or age. Nevertheless, our results revealed significant variations between the two groups in various aspects of autonomic function.
Firstly, HRV test, including E/I ratio, Valsalva ratio, and 30:15 ratio, demonstrated a statistically significant difference between ET patients and the control group, suggesting alterations in autonomic regulation in the ET patient group. These results differ from the previous work of Kim et al., [13] who found no significant differences in heart rate between ET patients and the control group. We can explain the difference in results by considering some limitations in the Kim et al., [13] study. Firstly, the ET-patient group had a higher prevalence of hypertension compared to the control group. Furthermore, patients were tested after stopping antihypertensive medications for a week, which raises concerns about the potential influence of drug withdrawal on the results. Another limitation is the discrepancy in sample sizes between the patient and control groups, and this may affect the interpretation of the study's findings.
The current study revealed notable variations in the SBP response during active standing and the DBP response during sustained hand grip in ET patients compared to control subjects, providing further evidence of autonomic dysfunction in ET patients. Interestingly, these results differed from a study conducted by Kim et al. [13], where they did not observe a statistically significant connection between cardiovascular autonomic dysfunctions (e.g., orthostatic hypotension, supine/nocturnal hypertension, non-dipping of blood pressure) and ET patients.
A more recently conducted exercise treadmill tests on two groups: individuals with essential tremor and a control group. Chronotropic index values, indicative of sympathetic nervous system function, were notably lower in the tremor group, suggesting impaired sympathetic activity. Initially (at one- and two-minutes post-test), the resting heart rate index values—indicative of parasympathetic system function—showed no significant difference between the two groups. However, these values were significantly higher in the tremor group at three, four-, and five-minutes post-test, suggesting reduced parasympathetic activity during the recovery phase. Thus, the study concludes that individuals with essential tremor may have abnormalities in cardiac autonomic functions, with evidence of deficits in both the sympathetic and parasympathetic systems [14]. These results confirm our findings.
Additionally, the results showed significant differences in the onset latencies and amplitudes of SSR in the palm and sole between the two groups. ET patients exhibited prolonged onset latencies and decreased amplitudes of SSR in both palm and sole, pointing towards autonomic involvement in ET.
A prospective study was conducted at Razi Hospital [15], including patients with ET. The sympathetic nervous system was assessed using the SSR, evaluated at all four limbs. The parasympathetic system was evaluated according to Ewing’s battery. The researchers reported neurophysiologic dysautonomia in 74% of ET patients, with reduced heart rate variability in 60% of the cases. Early parasympathetic dysfunction was observed in 86.7% of patients and definite dysfunction in 13.3%. Sympathetic dysautonomia was identified in 30% of patients. These findings confirm the high prevalence of autonomic dysfunction in ET, affecting both parasympathetic and sympathetic systems as assessed through electrophysiological methods. Our results are in alignment with these conclusions.
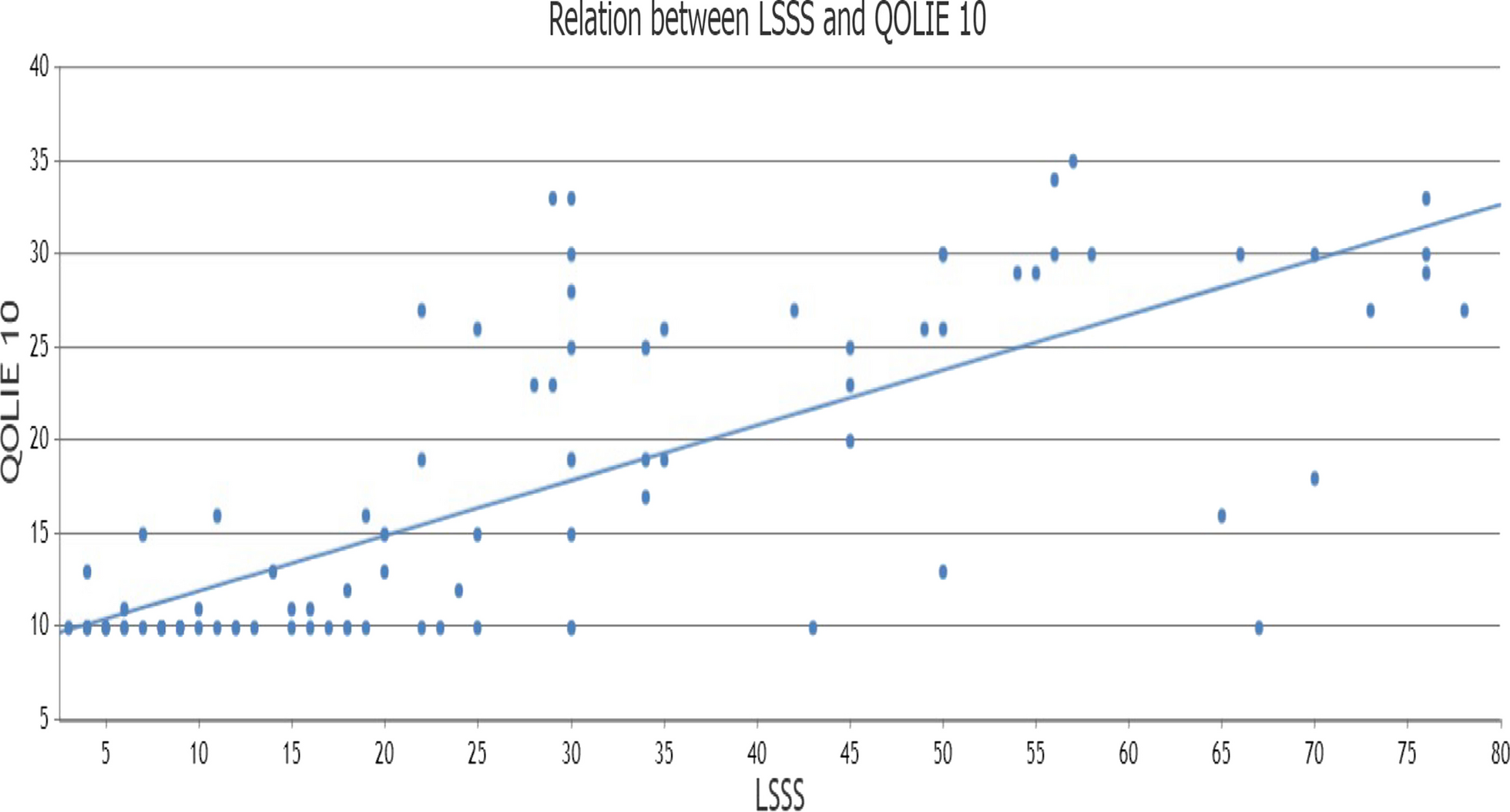
Moreover, we found significant correlations between the TRETRS and various autonomic function tests and the Ewing score. As the severity of ET increased, there was a greater impact on autonomic function tests. Notably, TRETRS showed a negative correlation with HRV tests, diastolic blood pressure response to sustained hand grip, and amplitudes of SSR in the palm and sole. Conversely, a positive correlation was observed between TRETRS and the onset latency of SSR in the palm and sole, as well as systolic blood pressure response to standing. These findings indicate that as the disease progressed, autonomic system involvement became more pronounced.
Reduced GABAergic function within the locus coeruleus, and subsequent adrenergic changes due to this GABAergic dysfunction in ET patients, have been proposed as potential explanations for autonomic dysfunctions, such as orthostatic hypotension. However, these hypotheses require validation through autopsy studies of ET patients, both with and without orthostatic hypotension [16].
Becktepe et al. demonstrated differences in the pupillary light response between early-onset and late-onset ET patients of the same chronological age. Their findings are interpreted as reflecting age-related biological differences between these two ET subgroups. This supports the concept that late-onset ET represents a distinct form of aging, affecting the brain stem, which in turn influences autonomic nervous system functions [17].




Comments (0)