In the general population, the prevalence of CM ranges from 1 to 4%; it affects women more frequently than males and peaks between the ages of 18 and 50. CM not only results in a lower QOL but also has a large socioeconomic cost due to lost productivity and working days [15]. Investigating the risk factors of headache frequency in CM is crucial for identifying associated factors and optimizing treatment paradigms. Only a small number of studies document CM remission [16].
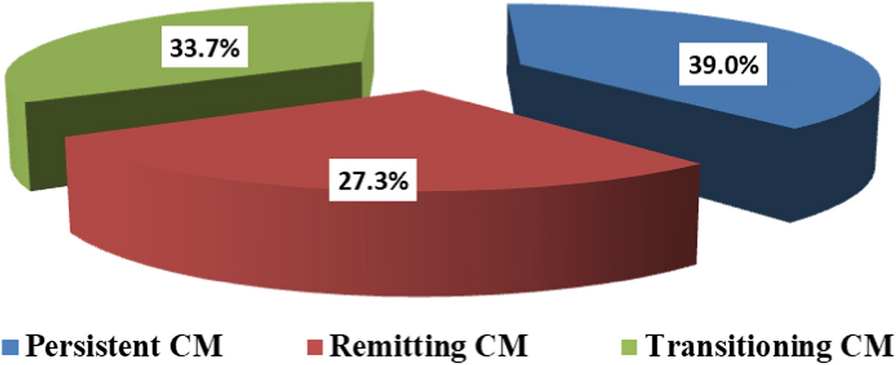
Findings in the current study indicate that more than one-third (39.0%) of sufferers with CM in a baseline year continue persistent over the subsequent 2 years of follow-up. Conversely, true remission occurs in only 27.3% of those with CM, and 33.7% had transitional CM.
Transitioning CM is defined as migraine that met CM criteria at baseline and either CM, low-frequency EM (LFEM), high-frequency EM (HFEM), chronic or episodic tension-type headache, probable migraine, no headache, or other episodic headache in subsequent years and did not meet persistent or remitting CM criteria [17].
Given that CM sometimes persists and sometimes remits, factors predicting remission were evaluated. Headache frequency per month, CM associated with allodynia, using medications as Topiramate or Beta-blockers, and smoking status were significant predictors for persistence or achieving remission among sufferers with CM.
Headache frequency was a significant independent predictor of CM remission, with higher headache frequency associated with lower rates of remission. This finding could be attributed to the fact that more frequent headaches were linked to more days with moderate-to-severe headaches, more frequent use of acute headache medications, more headache-related disability, and ultimately a lower QOL [18]. In contrast, a reduction in headache frequency may also translate into improvements in health-related QOL [19]. Thus, patients with higher headache frequency have a poorer outcome.
However, evidence from previous studies was contradictory. Similar findings were reported by [7, 20, 21] who reported that lower baseline headache frequency was a significant predictive factor for the remission of chronic migraine. Moreover, it was found to be linked to a decrease in migraine days at follow-up but also to an increased risk of allodynia and more drug use days [22]. Also, recently Henning and colleagues reported that there was a lower chance of remission for participants whose baseline headache frequency was higher (0.90, 0.84–0.97) [16].
Conversely, research showed that there was no difference in the incidence of headaches between those who responded and those who did not to preventive treatment [23], and higher baseline headache frequency did not predict treatment-induced remission of chronic migraine [24].
Evidence has accumulated that migraine progression and disability are influenced also by cutaneous allodynia, the perception of non-noxious thermal or mechanical stimuli as painful [25]. It was reported that allodynia affected 63% of migraineurs in the population and was associated with female sex, frequency, severity, and most of the diagnostic symptoms of migraine [26]. In the current study, the prevalence estimates of allodynia among our studied cases were 67.9%. Also, we observed that allodynia is more common and more severe in individuals with persistent migraine compared with those with remitting migraine. This finding was confirmed in the logistic regression analysis as we observed that patients with non-CM with allodynia (0–2) were more likely to remit (OR = 69.557, 95% CI: 4.013–1205.592, P = 0.004) compared to those with moderate to severe CM with allodynia (≥ 6). In line with this finding, Manack and colleagues stated that the absence of allodynia has been shown to be associated with remission [7], and Louter and colleagues reported that allodynia is more common in those with chronic migraine than in people with episodic migraine and suggests a higher risk of migraine chronification [22].
Medication overuse (use of acute medications on more than 10 or 15 days per month, depending on the medication class) is common among people with CM. For some people with migraine, despite taking greater amounts of acute headache medication, they develop an increase in monthly headache days [27]. In the current study, we observed that regular intake of analgesics was associated with persistent migraine. However, regression analysis revealed that medication utilization by class, and OTC/prescription overuse did not significantly predict CM remission. Similar finding was reported by Manack and colleagues [7].
Evidence for the efficacy of oral agents in CM is generally extrapolated from studies in patients with high-frequency EM [28]. Thus, preventive treatment is intended to facilitate the transition from CM to EM, but the real-world benefits of this remission have yet to be quantified. In the present study, the current use of preventive medications facilitated the achievement of remission. In the regression analysis model, we observed that those using Topiramate were more likely to achieve remission (OR = 12.561, 95% CI: 2.736–57.672, P = 0.001). Thus, we suggested that preventive medications may also increase remission rates, but effects may be offset by other unmeasured or inadequately measured confounders.
In line with the current study, Manack and colleagues reported that the use of preventive medications was associated with a lower rate of remission [7]. The author explains this finding as follows: persons with CM who receive preventive medication may be more likely to have other factors, such as high attack frequency, associated with a reduced chance of remission [7].
The most popular class of medications for treating migraines in prevention are beta-blockers, which can reduce migraine frequency by more than 50% with an efficacy of roughly 50%. The effectiveness of metoprolol, a selective beta1-blocker, and propranolol, a nonselective beta-blocker, has been repeatedly shown by evidence. Atenolol, nadolol, timolol, and bisoprolol are also shown to be effective [29]. This comes in agreement with the current finding as we observed that receiving Beta-blockers was effective in achieving remission among the studied cases.
Caffeine can cause migraine headaches by increasing urinary magnesium loss, most likely by inhibiting magnesium reabsorption. Caffeine may cause headaches by reducing magnesium levels, which affects neuromuscular conduction and nerve transmission and is beneficial in chronic pain syndromes including migraines. One probable migraine trigger is dehydration. Caffeinated coffee, in higher dosages, has an acute diuretic effect, which can lead to dehydration [30]. This could explain the current finding that drinking coffee was more prevalent among patients with persistent headache, and patients not drinking coffee were four times more likely to achieve remission in regression analysis model, with borderline significance. Similar finding was reported by previous literature [8].
It was discovered that smoking and migraines were related. A retrospective examination of data from the annual health survey revealed a positive correlation between the prevalence of migraines and daily smoking [31]. There is debate over the pathophysiology of smoking and nicotine use in the beginning of migraines, as both substances directly affect the central nervous system [32]. In the present study, smoking was found to be associated with persisting headache. Participants who did not smoke were more likely to experience remission of migraine. Similar finding was reported by Gong Q and colleagues [33].
Disability, anxiety, and depression are common risk factors of chronic migraine [34]. In the current study, we observed that patients with persistent headache suffered from higher disabilities, lower quality of life (QOL), and associated with other psychiatric comorbidities as depression, anxiety. This finding was supported by previous studies [35].
Manack and colleagues showed that disability is significantly influenced by persistence and remission. Remitted CM patients showed reductions in headache-related disability, but those with persistent CM showed increases in headache-related disability [7].
Patients with CM showed more impairment, a lower quality of life, and higher levels of anxiety and depression than those with EM, according to data gathered by the International Burden of Migraine Study (IBMS) from multiple countries in Western Europe, North America, and the Asia/Pacific areas [36, 37]. Also in line with the current study, the recent meta-analysis of Xu and colleagues reported that depression, anxiety are among modifiable risk factors for the transformation of EM to CM [38].
In fact, CM and depression are recognized risk factors for suicidal thoughts or behaviors in those who suffer from migraine [39, 40]. This finding highlights the need for proper prevention and management to avoid these catastrophic outcomes.




Comments (0)