This study is a prospective, cross-sectional, tertiary hospital-based study aiming to identify the profile of adult patients with new onset epilepsy in Zagazig University hospitals that support investigations, treatment of patients at reduced prices, provides medical consultation and inpatient services almost free of charge.
In our study 57% of the studied patients were males, and 43% were females, with male to female ratio of 1.3 to 1. The mean age in years (± SD) was 52.83 (± 17.33) with range from 19.0 years to 82.0 years. Educational level varied among studied patients as 9.0% were illiterate, 31.0% had primary school level, 42.0% had high school level, and 18.0% had college level. Regarding residence identity, 47.0% were from urban areas, and 53.0% were from rural areas. Regarding marital status 77.0% were married, and 33.0% were unmarried.
Middle-age group (aged from 40 to 65 years) showed higher prevalence (41%) of epilepsy than young adults (aged from 18 to 40 years) who showed prevalence of 26%, and older adults (aged more than 65 years) with prevalence of 33%.
In agreement with these results, Bhatia and colleagues [14] showed that male patients outnumbered female patients, 54.4% of the patients were males, and 45.6% were females, with an average age of 44.6 years, and the male to female proportion was 1.2 to 1. Similar results were reported by Kaur and colleagues [15] who stated that 65% were males, most of the patients (38%) were in the age group of 21 years–40 years and 41 years–60 years, only 9% were of < 20 years, and 15% were of more than 60 years.
Contrary to these results, Ali and colleagues [16] reported that the majority of patients were females (55.1%). On the other hand, Sheikh and colleagues [17] stated that both younger age group (25 years -34 years), and male patients showed higher prevalence. This difference in our study could be because most of the patients belonged to the middle-aged adult group (> 40 years to 65 years), and also may be because older adult patients (> 65 years) used not to seek medical advice as compared to other age groups.
In our study, 87% of the studied patients had no family history of epilepsy, and 13% had positive family history of epilepsy. That relatively higher percentage of absence of epilepsy family history in our study, is going with the relatively high percentage of presence of organic cerebral pathology (88%), and of having acquired etiology (87%) in our study. Which may be expected when the included patients are all having adult-onset epilepsy, as in our study.
There were 32.0% of the studied patients having focal epilepsy (of them, 11% had epilepsy with focal onset aware seizures, and 21% had epilepsy with focal onset seizures with impaired awareness), while 68.0% of the studied patients had generalized epilepsy (of them, 42% had epilepsy with generalized onset motor seizures and 26% had epilepsy with generalized onset non-motor seizures (absence)). In agreement with these results, Sheikh and colleagues (17) stated that among the participating subjects, generalized tonic–clonic seizures were the most common type of seizures (48.8%), followed by focal seizures with impaired awareness (14.6%).
This is in accordance with Kaur and colleagues [15] who carried out a study on 100 patients with adult-onset epilepsy and reported that the majority (59%) had generalized seizures. Out of rest 41 with focal seizures, 16 (39%) had focal aware seizures, 15 (36.6%) had focal seizures with impaired awareness, whereas remaining 10 (24.4%) had focal seizures with secondary generalization.
These results are different from Bhatia and colleagues [14] who had reported that the most common seizure type of seizure was generalized tonic–clonic seizures, present in 98.9% of patients, whereas focal seizures were seen in 1.1%, and the percentage of patients having generalized tonic–clonic seizures was more than those in our study, probably because all patients in their study were enrolled from emergency departments where most of the active epilepsy patients brought to emergency room are those having the grand mal presentation (generalized tonic–clonic seizures), particularly when they take the serial or status form.
In our study 47.0% of the studied patients had controlled seizure, and 53.0% had uncontrolled seizure. The mean (± SD) seizure frequency per month was 4.0 (± 3.15), with range from 1.0 to 15.0. The majority of the studied patients (61%) had 1 to 4 seizures per month, 30% had 5 to 8 seizures per month, and 9% had 9 to 15 seizures per month. Bhatia and colleagues [14] reported that the majority of their patients (92.2%) had one to five episodes of seizure per month, whereas 5.6% of patients were found to have six to ten episodes, and 2.2% were found to have 10 –15 episodes of seizure.
In our study 12.0% of the studied patients had normal computed tomography (CT) / magnetic resonance imaging (MRI) brain, and 88.0% had abnormal CT / MRI brain. Parallel to the results of our study, Bhatia and colleagues [14] showed that almost 72% had abnormal brain imaging and Sheikh and colleagues [17] stated that MRI showed abnormal findings in 59.7% of the patients.
Similar to our results, Mahmoud and colleagues [18] showed that abnormal findings in neuroimaging were detected among (75%) of adult-onset epilepsy patients. This can be going with the expected relatively higher percentage of organic cerebral pathology in adult-onset epilepsy as in our study inclusion criteria.
The findings of our study revealed that 57% of the studied patients had a within normal EEG, and 43% had abnormal EEG. In agreement with our study, Mahmoud and colleagues [18] found that electroencephalographic data were useful; where it detected abnormality in 37.5%, and Sheikh and colleagues [17] reported that EEG findings were abnormal in 52.8% of their patients. Furthermore, Kaur and colleagues [15] reported that 44% of their patients had an abnormal EEG record suggestive of seizure activity, whereas 56% of their patients had a normal EEG record. The results of our study are different from those of Hosalli and colleagues [19], who reported that out of 100 cases, EEG was done in 45 cases only as demanded by clinical situation. About 14% had an abnormal EEG record while the rest 31% (n = 31) had a normal EEG record. The difference is probably because of not performing EEG for all patients in their study.
In our study, 45% of studied patients had post-ictal confusion, 66% had post-ictal focal neurological deficit (hemiparesis in 33.0%, cranial nerve affection in 18.0%, language and speech dysfunction in 9.0%, and monoparesis in 6.0%). Of the studied patients, 43% had ictal sphincteric incontinence, 11% had ictal tongue biting, 5% had pot-ictal fever, and 5% presented in status epilepticus.
In our study 32.0% of the studied patients were hypertensive on treatment, 18.0% had chronic migraine, atrial fibrillation was found in 16.0% of patients, 14.0% were diabetics, 9.0% had dyslipidemia, 5% had coronary heart disease, 3.0% had chronic kidney disease, and 1.0% had chronic liver disease. In our study post-traumatic epilepsy was of higher percentage in male than female patients, and focal cortical dysplasia and mesial temporal sclerosis were higher in males. Arteriovenous malformations were significantly higher in females. Post-traumatic brain injury, focal cortical dysplasia, and mesial temporal sclerosis as causes of epilepsy were statistically significantly higher in males. Arteriovenous malformations were statistically significantly higher in females.
Regarding distribution of comorbidities in different age groups, our study revealed that hypertension was significantly higher in middle-aged adults’ group (40–65 years) than in other age groups. Atrial fibrillation, coronary heart disease, diabetes mellitus and dyslipidemia were significantly higher in older adults (> 65 years) age group than in other age groups. Also, chronic migraine was higher in young adults (18 years–40 years) age group than in other age groups.
Bhatia and colleagues [14] showed in their study that the majority of cases (81.1%) had no past history of medical diseases, whereas 7.7% had hypertension, 5.6% had diabetes. These figures are much lower than what is in our study, which may be attributed to differences in cultural and environmental factors, and in lifestyle and feeding habits, also it may be attributed to the much lower age range of their patients than ours, where two thirds of their patients aged from 13 to 55 years, while 74% of our patients aged from > 40 to > 65 years.
Our study revealed that post-stroke epilepsy was higher in older adults, and middle-age adults’ groups more than in young adults age group and intracranial neoplasms were of higher percentage in older adults age group than other age groups. In agreement with our findings, Mahmoud and colleagues [18] revealed that post-stroke epilepsy is the most common etiology for adult new-onset epilepsy (44.17%), and the highest prevalence was in the older adults (> 65 years) age group (65.28%).
This is in accordance with study of Bhatia and colleagues [14] who illustrated that new-onset seizures have different etiologies in different age groups. In the middle-age group (between 36 and 55 years), cerebrovascular accidents were the dominant etiology present in 36.7% of the patients. The second most common etiology in this age group was CNS infection. The third most common cause was metabolic abnormalities in this age group. In the older age group (above 55 years), the most dominating etiology was cerebrovascular accident, followed by infective etiology.
Stroke was shown to be the most prevalent cause of seizures in older adults, according to a study by Kaur and colleagues [15].
According to study by Hirani and colleagues [20], CNS infections (38%), stroke (30%), and idiopathic seizures (25%) were the most common causes of adult-onset seizures. Infective causes of epilepsy were predominant in young patients, and stroke became the dominant cause as age increased. Kaur and colleagues [15] documented that in their studied 23 patients with post-stroke seizures, the highest prevalence was among individuals aged more than 40 years (95.6%). Idiopathic seizures were more common in younger adults (68.1%) aged less than 40 years, followed by CNS infections (66.6%). Metabolic causes and brain tumors were the cause of seizures in minority of cases.
Our findings regarding laboratory investigations revealed that all the studied patients had normal serum electrolytes (sodium, potassium, calcium, magnesium), and serum antiepileptic drugs (AEDs) level (valproate, phenytoin, carbamazepine) was significantly lower in patients with severe seizures (measured by LSSS) than in those with mild, and moderate seizures. Contrary to our findings, Bhatia and colleagues [14] reported that the most common metabolic abnormality found was hyponatremia in 6.3% of patients, followed by hypoglycemia in 2.3% of patients, and the least common was hypocalcemia in 0.9% of patients. Also, Mahmoud and colleagues [18] revealed that epilepsy patients with new-onset seizure had significant findings in their metabolic profile included 10% of patients with hypocalcemia, 6.67% of patients with hyponatremia, 4.17% of patients with hypokalemia, 5.83% patients with hyperglycemia and 2.5% of patients with hypoglycemia.
Rayamahji and colleagues [21] showed that the most common cause of seizures was hyponatremia. According to a report in the United States of America, the prevalence of hyponatremia in the emergency department was 2.7%. Also, a survey in Taiwan performed by Hao and colleagues [22] showed that prevalence of hyponatremia was 2.9%. The reason for this difference is that acute symptomatic seizures within 24 h in documented severe selected metabolic derangements were excluded from our study (Methods, Exclusion Criteria).
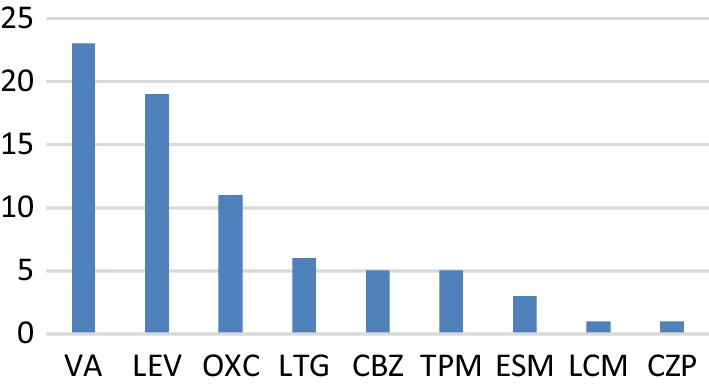
Our findings regarding AEDs revealed that there were 49% of the studied patients regularly on a single antiepileptic drug, and 51.0% on multiple AEDs (40.0% on two AEDs, 9.0% on 3 AEDs and 2.0% on 4 AEDs). Also, 42.0% were on old AEDs, 41.0% were on newer AEDs, and 17.0% were on both old and new AEDs. Levetiracetam was the first line monotherapy in 40.0% of our patients, 34.0% were on valproate, 32.0% were on carbamazepine, and 20% were on phenytoin.
In agreement with our results, Lezaic and colleagues [23] mentioned that levetiracetam had better tolerability when compared with other AEDs in post-stroke epilepsy in the older adults, and was the most commonly used as first line therapy. Similarly, Martin and colleagues [24] demonstrated that the most commonly prescribed initial antiepileptic drug was levetiracetam in 45.5% of patients, followed by phenytoin in 30.6%. These results were compatible with Thurman and colleagues [25] who reported that levetiracetam was the most common antiepileptic drug prescribed for initial monotherapy.
In contrary to these results, an old study by Pugh and colleagues [26] which showed that phenytoin was the most commonly prescribed antiepileptic drug in older adult individuals with new-onset epilepsy.
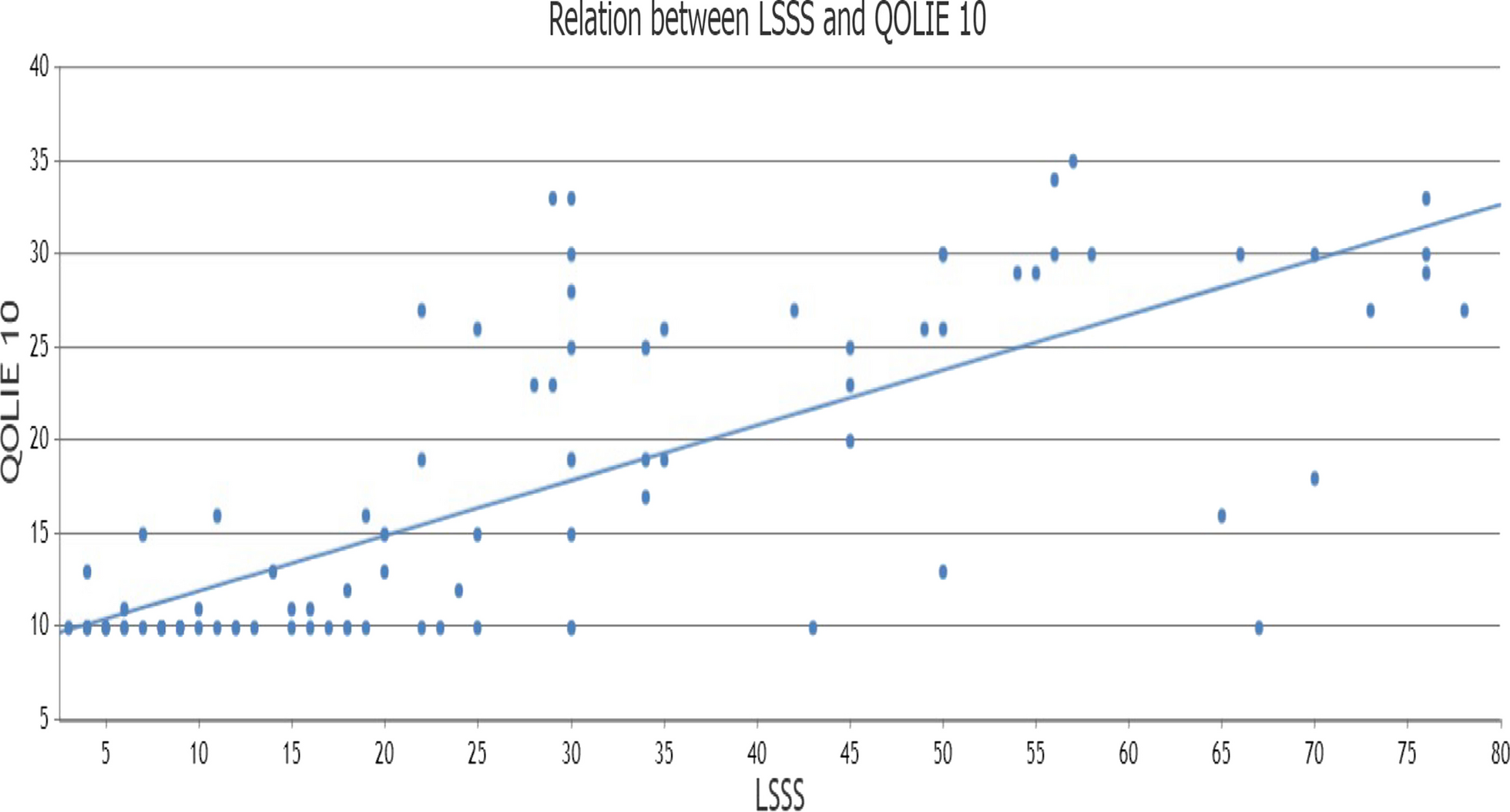
Among our patients, 47% had mild seizure severity, 26% had moderate, 17% had severe, 10% had very severe seizures, and older adults group had higher scores in Liverpool Seizure Severity Scale than other age groups. Another important finding in our study was that patients regularly on AEDs polytherapy had significantly more score on LSSS than those on monotherapy.
Viteva and colleagues [11] done a study on 70 adult patients with refractory epilepsy, and 70 patients with pharmaco-sensitive epilepsy, and evaluated the seizure severity using LSSS. Severe seizures were found in 18 (30.51%) participants, moderate in 32 (54.24%), and mild in 8 (13.56%) participants.
In our study, concerning Quality of Life In Epilepsy-10 Questionnaire (QOLIE-10) score, 70% of the studied patients had average quality of life, while 30% had impaired quality of life. Patients with impaired quality of life had more seizure frequency, less seizure control, and higher seizure severity. Also, they had more abnormal EEG findings and were mostly treated by AEDs polytherapy than those with average life quality.
Similar to the results of our study, a study in Ethiopia done by Muche and colleagues [27] on 354 patients showed that the mean QOLIE-10 score was 19.85 (± 8.35), and 54.8% of participants had a good quality of life.
In agreement with the results of our study, Espinosa and colleagues [28] conducted a study on 220 epileptic patients in low-income countries and found that the score of the QOLIE-10 was significantly affected by epilepsy and multiple AEDs intake which adversely affected quality of life.
Alexander and colleagues [29] mentioned that patients on polypharmacy had worse QOLIE-10 scores even after controlling their seizure status. Harden and colleagues [30] examined a group of females aged from 18 to 45 years with refractory epilepsy, and found that even when controlling their depression, seizure severity was inversely correlated with quality of life.
Bautista and colleagues [31] indicated that quality of life of patients with epilepsy was adversely affected by seizure severity.
Furthermore, Sancho and colleagues [32] indicated that the quality of life in patients with severe seizures has been consistently shown to be worse than for those with mild or moderate seizures.
However, the current study may be limited by the relatively small sample size So, further larger studies need to be done on choosing the best antiepileptic drugs in cases of adult-onset epilepsy taking patients’ age, sex, occupation, and comorbidities in consideration, with follow up of their effectiveness in prevention of recurrence, and adverse effects.




Comments (0)