
Remember me



We conducted a retrospective observational study in old stroke patients who underwent inpatient rehabilitation at Institute Guttmann between January 2015 and August 2022.
Eligible participants were adult patients over the age of 60 with ischemic or hemorrhagic stroke, who underwent at least 4 weeks of inpatient multidisciplinary neurorehabilitation within the first 6 months following a stroke. Patients presenting stroke secondary to traumatic brain injury, brain tumors or infections were excluded from the study.
Data of eligible patients were collected through the Comprehensive Information System of Institute Guttmann (SIIG) [9]. Missing data were collected from clinical records.
The Research Ethics Committee of the Fundacio La Unió approved the request to waive the documentation of informed consent. The study has been carried out in accordance with the recommendations of the Declaration of Helsinki. The study conforms to the STROBE standards for observational studies (www.strobe-statement.org).
The Institute Guttmann is a tertiary healthcare center in Barcelona (Spain) specializing in intensive rehabilitation of patients with neurological diseases. Older stroke patients have access to the rehabilitation programs through private health insurance or privately.
We collected the following variables: demographic data [age and sex], stroke type [ischemic or hemorrhagic], stroke location [right, left or bilateral], territory of ischemic stroke [total anterior circulation infarcts (TACI), partial anterior circulation infarcts (PACI), lacunar circulation infarcts (LACI), and posterior circulation infarcts (POCI)] according to the Oxfordshire Community Stroke Project (OCSP) [10], revascularization treatment for ischemic stroke (intravenous thrombolysis; mechanical thrombectomy; or both), complications of revascularization treatment [hemorrhagic transformation], type of hemorrhagic stroke [intracerebral hemorrhage (ICH) and subarachnoid hemorrhage (SAH)], complications of hemorrhagic stroke [subarachnoid extension of ICH, intraventricular extension or hydrocephalus], surgical treatment of hemorrhagic stroke [decompressive craniectomy or ventricular drainage].
Clinical scales have been used to assess: stroke severity on admission using the National Institute of Health Stroke Scale (NIHSS) [11]; functionality on admission and discharge based on the motor and cognitive domains of the Functional Independence Measure (FIM) scale [12]; the degree of independence using the Modified Rankin Scale (mRS) [13]; and dysphagia severity was assessed on the Functional Oral Intake Scale (FOIS) [14].
Language was evaluated by speech therapists and neuropsychologists using the Test Barcelona [15] and the PMR test, which evaluates the phonological verbal fluency for the letters P, M, R and represents the Spanish version of the FAS letter fluency task [16]. For the current study, three subtest were employed as screening tools for impaired verbal repetition, naming, and comprehension, whereas the PMR test was used to evaluate verbal fluency.
Obesity was defined as Body Mass Index (BMI) > 30 kg/m2 according to the WHO criteria.
Cardiovascular risk factors: diabetes mellitus, dyslipidemia, hypertension, atrial fibrillation, ischemic heart disease, previous stroke, obesity, current smoking or alcohol consumption were recorded as binary variables (“yes” = 1; “no” = 0).
Medication use during hospitalization: antidepressants, antipsychotics, antiepileptics for seizure treatment, antiepileptics for neuropathic pain (gabapentin, pregabalin), and benzodiazepines were recorded as binary variables (“yes” = 1; “no” = 0).
Patient safety-related complications during hospitalization: pressure ulcers, falls, hospital acquired infections (respiratory, urologic, skin and soft tissues), presence of multi resistant infections were recorded as binary variables (“yes” = 1; “no” = 0).
All patients underwent rehabilitation tailored to their neurological sequelae, according to their functional state and tolerance, guided by goals set by the rehabilitation team. Patients underwent two to four daily sessions of physiotherapy and occupational therapy (60 min) 6 days/week, one daily session of individualized speech and swallowing therapy (30 min) 3 times/week, and one daily session of neuropsychological training (60 min) 3 times/week. It is important to note that this description does not constitute an intervention study.
Outcome variables were m-FIM, c-FIM, FOIS at discharge and the hospital length of stay.
Aphasia improvement at discharge was recorded as binary variable for specific domains (expression, comprehension, repetition and naming) (“improvement” = 1; “no improvement” = 0).
We calculated functional gain, efficiency, and effectiveness, which allow evaluating the absolute change in functional scores as well as the time-dependent and the state-dependent improvement in functional scores. FIM gain = FIM at admission-FIM at discharge. FIM efficiency = FIM gain/LOS. FIM effectiveness = FIM gain/(maximum FIM score- FIM score on admission). FIM gain, efficiency and effectiveness were calculated for the motor and cognitive sub-scores [3]. Similarly, FOIS gain = FOIS on admission-FOIS at discharge. FOIS efficiency = FOIS gain/LOS. FOIS effectiveness = FOIS gain/(maximum FOIS score−FOIS score on admission). Dysphagia at discharge was recorded as binary variable.
Statistical analyses were conducted with a commercial Statistical Package for Social Sciences version 16.0.1 (SPSS Inc., Chicago, IL, USA, 2007).
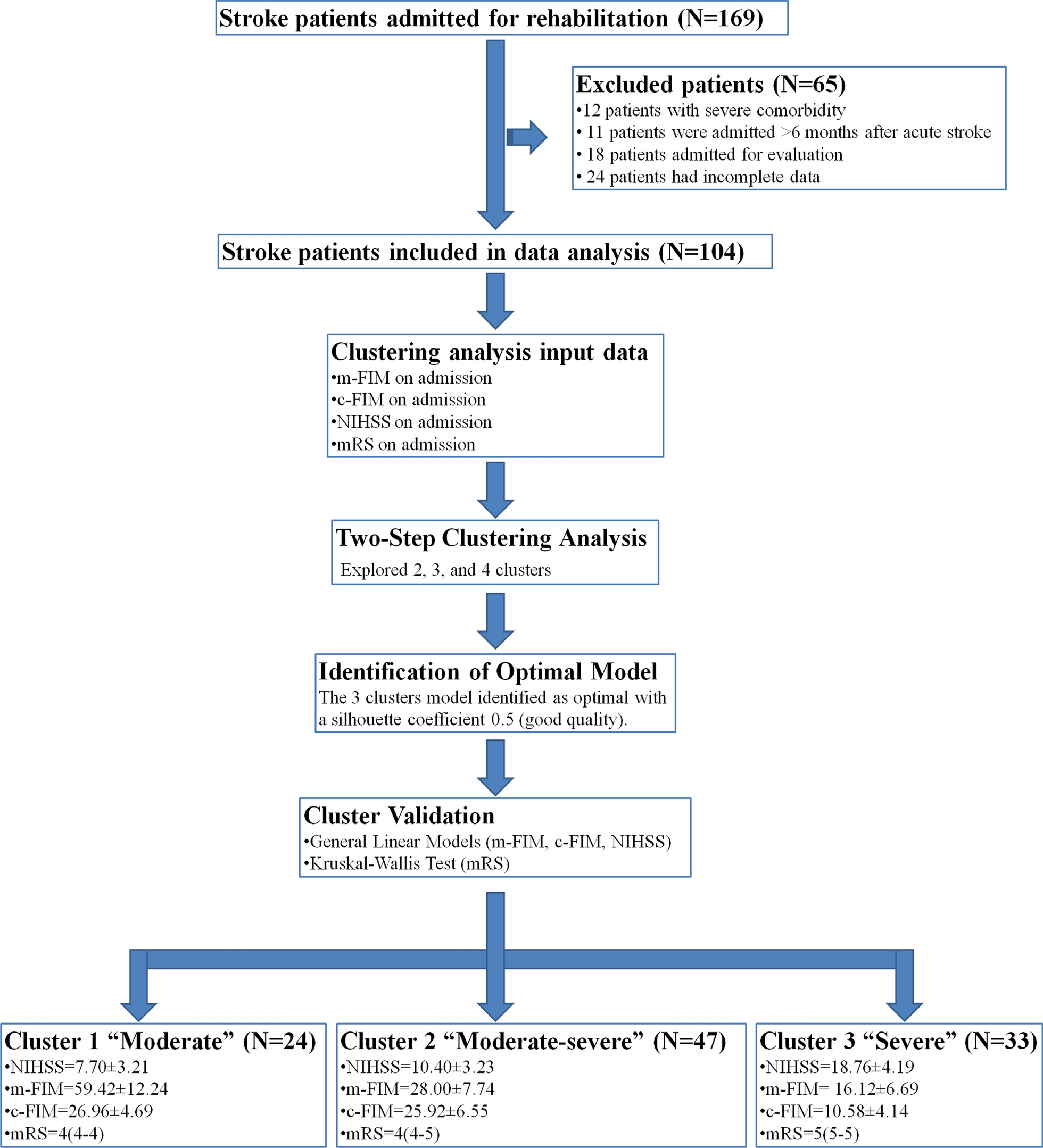
Descriptive statistics were used for demographic and clinical characteristics. Continuous parametric variables are presented as Mean ± SD or median [25th–75th percentile], whereas categorical variables are presented as numbers and percents. Shapiro–Wilk’s test was used to examine the normality of distribution. To identify possible rehabilitation profiles, we conducted two step clustering analysis including standardized m-FIM, c-FIM, NIHSS and mRS on admission, which were reported as predictors of rehabilitation outcomes in multiple studies and are considered relevant functional and independence measures for admission decision-making process. We explored possible grouping of patients into two, three or four clusters. The three clusters model was the optimal number of clusters with a silhouette coefficient 0.5 (good quality). To validate the clusters, we compared the dependent variables between cluster using general linear models for parametric data (m-FIM, c-FIM, NIHSS) or the Kruskal–Wallis test for nonparametric data (mRS) (Fig. 1). A General linear models with Bonferroni post hoc analyses were used to compare baseline parametric variables (age and BMI) as well as to compare rehabilitation outcomes between clusters (m-FIM and c-FIM at discharge with admission score as covariate). We used the Kruskal–Wallis test with the Mann–Whitney U test as post hoc to compare nonparametric variables (mRS and time since stroke to admission) and outcomes (gain, efficiency and effectiveness of m-FIM, c-FIM and FOIS) between groups. The χ2 test was applied to test relationships between categorical variables and clusters.
Fig. 1
Methodological approach: clustering analysis to identify rehabilitation profiles. m-FIM: the motor Functional Independence Measure; c-FIM: the cognitive Functional Independence Measure; NIHSS: the National Institutes of Health Stroke Scale; mRS: Modified Rankin Score
We performed simple regression analyses to study the relationship between functional outcomes (m-FIM, c-FIM) and the LOS (days) and dependent variables and sociodemographic (age, gender) and clinical characteristics (stroke characteristics and severity, functional variables on admission, associated comorbid conditions, inhospital complications or medication use) as independent variables.
Comments (0)