
Remember me



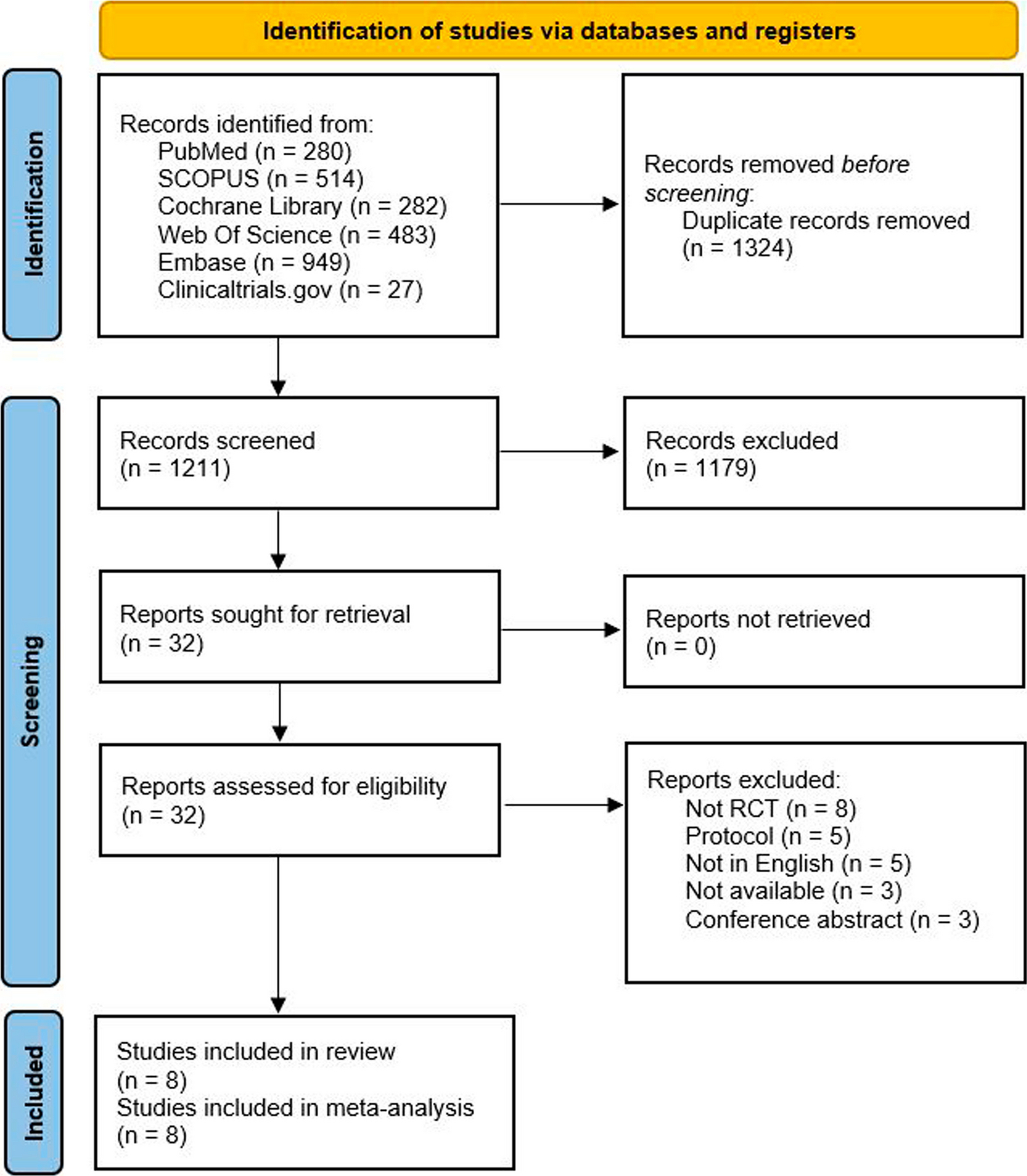
A total of 2,535 studies were retrieved from six different databases; PubMed (n = 280), SCOPUS (n = 514), Cochrane Library (n = 282), WoS (n = 483), Embase (n = 949) and Clinicaltrials.gov (n = 27). After removing duplicates, 1211 studies were eligible for the title and abstract screening. We performed full-text screening for 32 studies, and eight studies [20, 23,24,25,26, 30,31,32] were included in our meta-analysis. Figure 1 shows the PRISMA flow diagram of study search and selection.
Fig. 1
Our meta-analysis pooled data from 4964 patients from eight clinical trials. The mean age was 41.5 years, and most of them were females (84%). The mean migraine illness duration was 20 years. The general and baseline characteristics of the included studies and population are shown in Tables 1 and 2.
Table 1 Summary of the included studiesTable 2 Baseline characteristics of the included studiesResults of the quality assessmentMost of the included trials were judged as low risk regarding first six domains. Only the study by Oakes et al. [26] did not report adequate data regarding the randomization and allocation processes; So, it was put at unclear risk of bias. However, all studies may have other bias as they funded by pharmaceutical companies. Figure 2 shows the summary of the quality assessment results.
Fig. 2
Risk of bias summary and graph
Analysis of the outcomesChange of migraine headache days after one monthEpisodic migraineGalcanezumab 120/150 mg was evaluated by seven studies [20, 24,25,26, 30,31,32]. Galcanezumab 120/150 mg significantly reduced MHDs than placebo after one month; MD = -2.13, 95% CI [− 2.75, − 1.52], p < 0.00001. The pooled analysis was heterogeneous (p = 0.0007, I2 = 74%) and could not be solved by sensitivity analysis. As for galcanezumab 240/300 mg, it was reported by four studies [20, 26, 31, 32]. Galcanezumab 240/300 mg significantly reduced MHDs after one month; MD = − 1.88, 95% CI [− 2.37, − 1.40], p < 0.00001. The analysis was homogeneous; p = 0.25, I2 = 27%. Figure 3
Fig. 3
A forest plot of the change in the migraine headache days after one month
Chronic migraineThis outcome was reported by two studies [23, 25]. Galcanezumab 120 mg significantly reduced MHDs after one month; MD = − 2.62, 95% CI [− 3.82, − 1.42], p < 0.0001. The pooled analysis was homogeneous, p = 0.24, I2 = 28%. Figure 3
Change of migraine headache days after two to five monthsGalcanezumab 120/150 and 240/300 mg significantly lowered MHDs in episodic migraine patients after two, three, four, and five months compared with the placebo; p < 0.05. Additionally, 120 and 240 mg galcanezumab significantly lowered MHDs in chronic migraine patients after two and three months than placebo; p < 0.05, Figs. 4, 5, 6, 7.
Fig. 4

a A forest plot of the change in the migraine headache days after two months before sensitivity analysis. b A forest plot of the change in the migraine headache days after two months after sensitivity analysis
Fig. 5
A forest plot of the change in the migraine headache days after three months
Fig. 6
A forest plot of the change in the migraine headache days after four months
Fig. 7
A forest plot of the change in the migraine headache days after five months
Change of migraine headache days after six monthsThis outcome was reported by three studies [20, 31, 32]. Galcanezumab 120 mg significantly decreased MHDs after six months in episodic migraine patients; MD = − 1.99, 95% CI [− 2.53, − 1.44], P < 0.00001. The pooled data was homogeneous; p = 0.3, I2 = 17%. Also, 240 mg galcanezumab significantly decreased MHDs after six months in episodic migraine patients; MD = − 2.28, 95% CI [-3.17, − 1.39], p < 0.00001. The pooled analysis was heterogeneous p = 0.05, I2 = 67%. Figure 8a Heterogeneity was solved after the exclusion of Sakai et al. [31]; p = 0.77, I2 = 0%. The pooled analysis remained significant; MD = -1.83, 95% CI [− 2.42, − 1.24], p < 0.00001, Figure 8b.
Fig. 8
a A forest plot of the change in the migraine headache days after six months before sensitivity analysis. b A forest plot of the change in the migraine headache days after six months after sensitivity analysis
Change in monthly migraine headache days (Months 1–3)Episodic migraineThis outcome was reported by three studies [24, 25, 30]. Galcanezumab 120/150 mg significantly reduced the monthly MHDs after one to three months; MD = − 1.87, 95% CI [− 2.60, − 1.14], p < 0.00001. The pooled analysis was heterogeneous p = 0.06, I2 = 64%. Fig S1a This was solved after excluding Dodick et al. [30]; p = 0.24, I2 = 28%. The pooled data remained in favor of galcanezumab; MD = − 1.56, 95% CI [− 2.16, − 0.96], p < 0.00001, Fig. S1b.
Chronic migraineThis outcome was reported by two studies [23, 25]. Galcanezumab 120 mg significantly lowered the monthly MHDs after one to three months of usage; MD = − 2.86, 95%CI [− 4.16, − 1.57], p < 0.0001. The analysis was homogeneous p = 0.22, I2 = 34%, Fig. S1.
Change in monthly migraine headache days with acute medication useEpisodic migraineTwo studies [24, 25] evaluated the 120 mg galcanezumab for 1–3 months. Galcanezumab 120 mg significantly decreased the monthly MHDs with acute medication use after one to three months; MD = -2.25, 95% CI [-3.25, -1.25], p < 0.00001. The pooled analysis was heterogeneous; p = 0.05, I2 = 74%. Another two studies [20, 31] evaluated the 120 mg galcanezumab after one to six months of usage. It showed a significant reduction; MD = − 2.32, 95% CI [− 3.40, − 1.25], p < 0.00001. The pooled analysis was heterogeneous; p = 0.02, I2 = 82%. As for galcanezumab 240 mg, two studies [20, 31] reported a significant reduction after one to six months of usage; MD = − 2.51, 95% CI [− 3.10, − 1.20], p < 0.00001. The pooled analysis was heterogeneous; p = 0.02, I2 = 82%. The heterogeneity of this outcome could not be solved by sensitivity analysis, Fig. S2.
Chronic migraineThis outcome was reported by two studies [23, 25]. Galcanezumab 120 mg significantly lowered the number of monthly MHDs with acute medication use after one to three months; MD = -3.09, 95% CI [-4.53, -1.65], p < 0.0001. The data were homogeneous; p = 0.13, I2 = 57%, Fig. S2.
Response ratesEpisodic migraineCompared with placebo, galcanezumab 120 mg significantly increased the 50%, 75%, and 100% response rates of episodic migraine after one to three months (RR = 1.9, 2.65, 4.19) and one to six months (RR = 1.78, 2.02, 2.42), respectively. Additionally, the galcanezumab 240 mg significantly increased the 50%, 75% and 100% response rates of episodic migraine after one to six months (RR = 1.72, 2.04, 2.51), respectively, Fig. S3–S5.
Chronic migraineGalcanezumab 120 and 240 mg significantly enhanced the 50% and 75% response rates of chronic migraine patients after one to three months than placebo; p < 0.05. In contrast, there were insignificant results with galcanezumab 120 or 240 mg regarding the 100% response rate of chronic migraine patients after one to three months; p > 0.05, Fig. S3–S5.
Safety outcomesMost of the included trials reported the incidence of adverse events. Regarding injection site outcomes, the results were significantly higher with galcanezumab 120 mg group. This includes erythema; RR = 3.76, 95% CI [1.91, 7.40], reaction; RR = 6.44, 95% CI [2.10, 19.77], pruritis; RR = 26.7, 95% CI [7.27, 97.93], and swelling; RR = 7.17, 95% CI [2.22, 23.17]. Also, these adverse events were higher with the galcanezumab 240 mg group except for injection site reaction, which showed higher with galcanezumab 120 mg only. Any adverse events were noticed higher with galcanezumab 120 and 240 mg groups. Furthermore, serious adverse events and adverse events that led to discontinuation were higher with galcanezumab 240 mg only; RR = 3.12, 95% CI [1.08, 9.04] and RR = 2.59, 95% CI [1.06, 6.35], respectively. The rest of adverse events showed no variation between galcanezumab and placebo groups. Table 3 and Fig. S6–S19.
Table 3 Adverse events summary of patients with episodic migraine
Comments (0)