Starting with clinical data as a clue to differentiate NMOSD patients from RRMS patients; NMOSD patients are older than RRMS patients at the onset of illness that is in line with Pandit and colleagues [19], while in a more recent study conducted by Lucía Romero-Pinel et al. [20] the age at onset RRMS has increased over the last five decades.
Regarding clinical severity and disability data, our results demonstrated that NMOSD patients had higher EDSS than RRMS patients with a significant P value = 0.0001, these results are in agreement with Juryńczyk et al. [21].
Comparing the most common affected domain in NMOSD and RRMS patients, we found that pyramidal was the most affected domains in both (96.7% and 83.3%, respectively) while 76.7% of NMOSD patients had visual affection on the other hand 50% of RRMS patients had visual affection, there was a high significant difference between both groups, P < 0.0001. Many studies supported our finding [22, 23].
For the second time in our study, our results revealed that the burden of illness in NMOSD is greater than that in RRMS as in NMOSD with relapse, among 15 patients, relapses were poly-symptomatic in 60% of patients and monosymptomatic in 40%. While among 15 patients in RRMS with relapse, relapses were monosymptomatic 60% and poly-symptomatic 40%.
Coming to radiological findings among our participants; in NMOSD patients with relapse, only four patients showed T2 lesions in the last MRI brain on the other hand, all RRMS patients in remission, showed T2 lesions in MRI brain and all patients in group RRMS with relapse showed new lesions.
Eighty presents of NMOSD group a patients had MRI spine lesions more than three vertebral segments in comparison to 9.1% of patients in RRMS in remission.
Regarding multiple sclerosis, disruption of the BBB is one of the underlying pathogeneses, which follows massive infiltration of T cells forming demyelinated plaques. Dysfunction of the BBB is also reported in neuromyelitis optica spectrum [24]. When anti-AQP4-IgG obtained from a NMOSD patient and administered to mice, lesions of perivascular astrocyte were noticed, indicating the dysfunction of BBB by impairing the expression of tight junction proteins [25].
Our results matched with that Collins and colleagues and Filippi et al. [26, 27] who proved the utility of MRI in demyelinating disease diagnosis.
To our knowledge this is the first study to compare serum glutamate level between NMOSD and RRMS patients, and shows that the level of glutamate was significantly higher in NMOSD patients without relapses when compared to MS patients without relapses with P = 0.005, it is a cheaper, easy and less invasive adjuvant tool for differentiation that may be of help especially in cases of AQ4 negative NMOSD; however, no significant difference was found between NMOSD and RRMS patients with relapses.
The higher glutamate level in NMOSD patients in remission could be related to the marked impairment of glutamate uptake by astrocytes found in NMOSD, and this NMOSD astrocytopathy is distinguishable from the immunopathology of multiple sclerosis.
Al Gawwam et al. [28] found a significant increase in serum glutamate in MS patients without relapse when compared to healthy controls. Other MS studies have also demonstrated increased levels of glutamate in CSF [29] or by using MRS [30]. The involvement of glutamate in the pathogenesis of MS could represent a secondary pathophysiological mechanism leading to demyelination and neuroaxonal damage.
As glutamate level will decline over time that might explain the presence of significant difference of serum glutamate between RRMS patients with and without relapses and the absence of such difference between NMO patients with and without relapses and between NMOSD patients with relapses and RRMS patients with relapses.
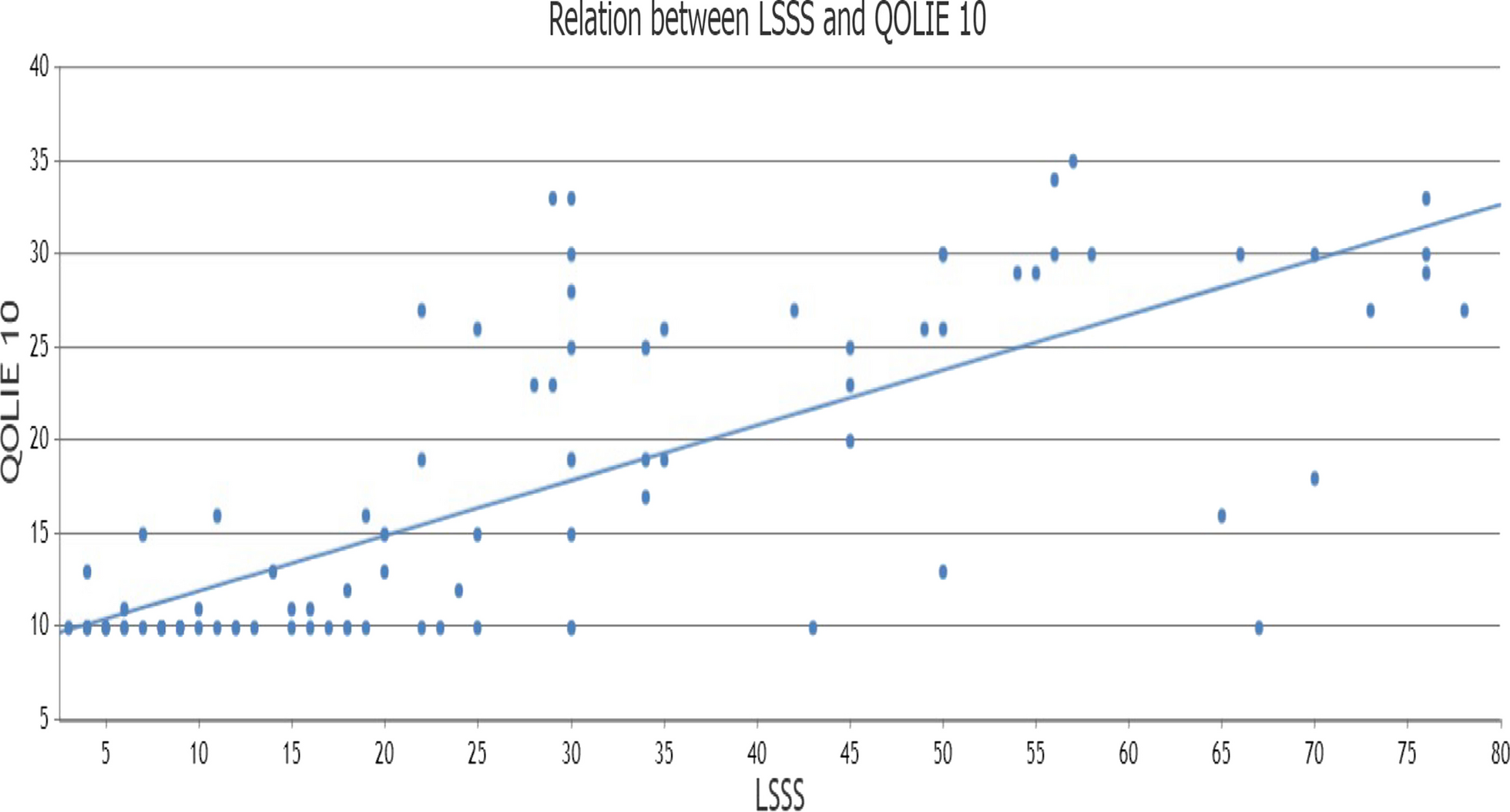
In RRMS patients without relapses, there was a significantly positive correlation between glutamate serum level and EDSS (r = 0.615, P < 0.05), but no such correlations were found in MS patients with relapses. This finding is consistent with an earlier study in Westall et al. [31].
Furthermore, the study in [30], which used MRS to evaluate the contribution of glutamate toxicity in MS, showed a correlation between increased levels of glutamate and EDSS, as they found that excess glutamate was associated with accelerated rate of neuroaxonal integrity, brain volume loss and worsening of clinical outcomes.
Using receiver operating characteristic (ROC) curve and AUC, the cut-off value of glutamate serum level for differentiation between NMOSD patients in remission and RRMS patients in remission was > 10.3 μg/mL with sensitivity 86.7% and specificity 60%, and the cut-off value of glutamate serum level for differentiation between RRMS patients in remission and RRMS patients with relapse was > 12.6 μg/mL with sensitivity 93.33% and specificity 80% (P value < 0.001). Validity analysis in another study stated that cut-off values of 17.5 μg/mL for glutamate and 75.2 nmol/mL for nitric oxide can predict occurrence of relapse [32].




Comments (0)