PPB is a rare pediatric pulmonary malignancy [1]. In 1994, Dehner established the current disease concepts as: type I, purely cystic lesion; type II, intermediate between types I and III; and type III, predominantly solid lesion [2].
Type I PPB is understood to show better prognosis than type II or III [2, 3]. However, with or without chemotherapy, 10% of type I PPB cases may progress to type II or III after surgical resection [3].
The similarities of PPB and between CPAM have been discussed [4,5,6]. In 2002, Stocker proposed the new disease concept of CPAM, which was classified according to the site of lesion development in the tracheobronchial tree [6], from congenital cystic adenomatoid malformation (CCAM), which had been classified according to histomorphology [7]. In particular, CPAM type 4 is derived from distal acini and is itself uncommon (~ 10% of the CPAM cases) [6], so differentiation from cystic type I PPB based only on appearance may difficult. As a result, pathological diagnosis becomes extremely important [5].
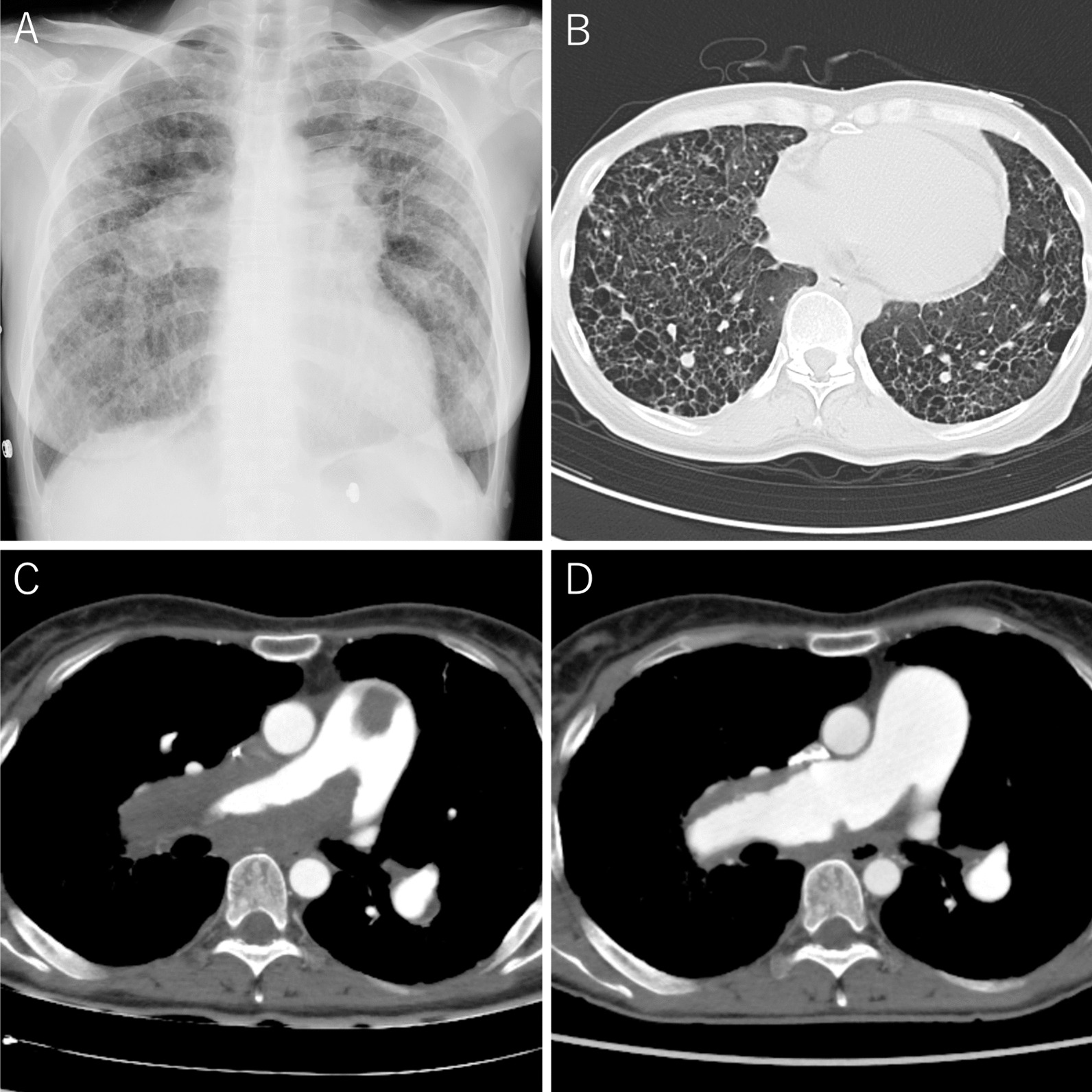
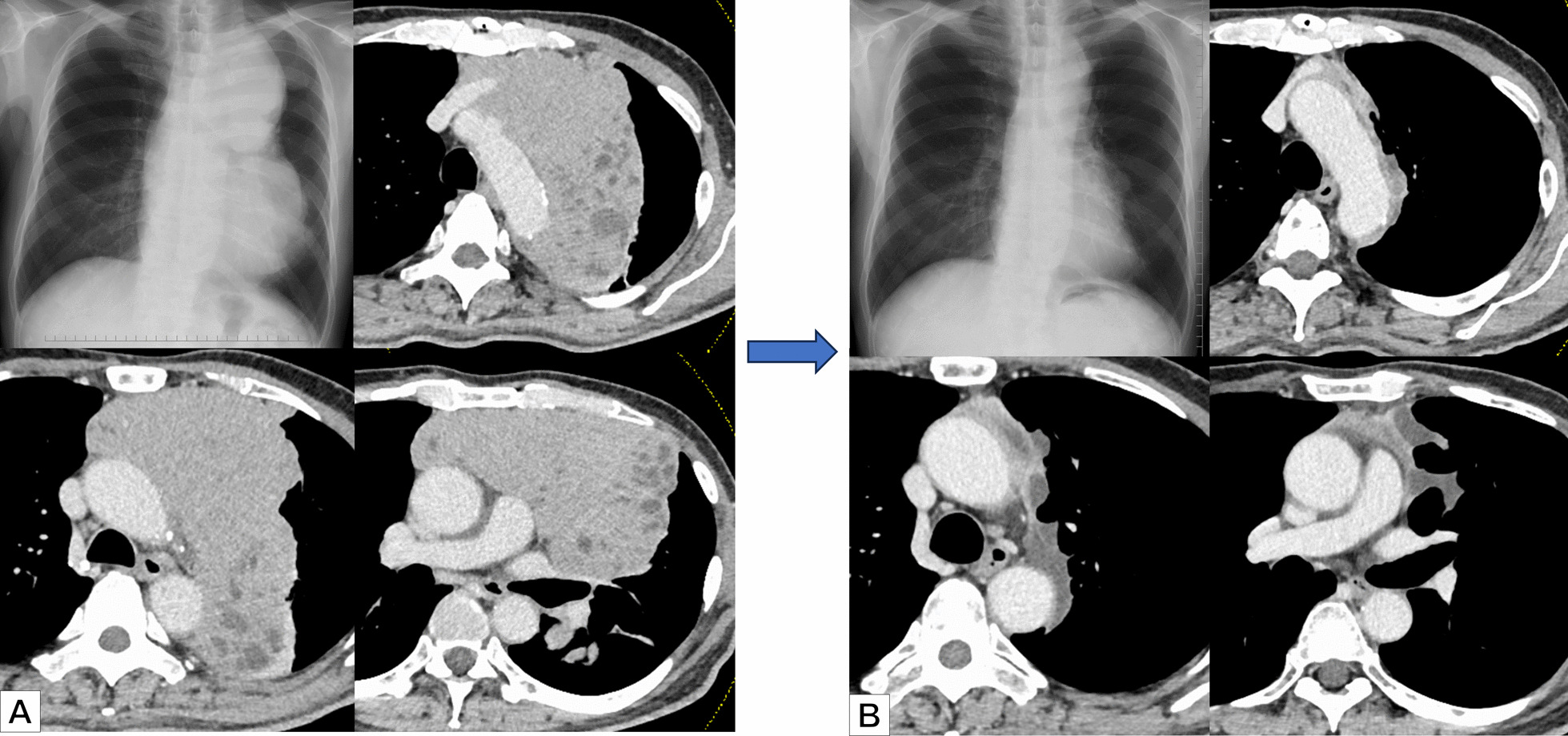
The patient in this case presented with respiratory failure due to compression of the mediastinum by a space-occupying tumor rather than pneumothorax, so resection through thoracotomy was performed. Feinberg et al. proposed a therapeutic algorithm for cystic lung disease, suggesting that surgical treatment be performed if symptoms are present [8], while keeping malignancy in mind during those surgical procedures.
In this case, 5 courses of VAC chemotherapy were administered because rupture had occurred and tumor cells were also found at the diaphragm adhesion site. Pneumothorax due to tumor rupture is one of the problems with cystic PPB lesions [9, 10], but possibly due to the small number of cases reported to date, detailed comparison of long-term prognosis between ruptured and non-ruptured cases in type I PPB has been not described.
In 2009, DICER1 gene was identified as the gene responsible for the onset of familial PPB [11]. Mutations in DICER1 cause abnormalities in proteins that produce micro ribonucleic acids (RNAs) involved in cell proliferation, apoptosis, and cell differentiation, leading to the development of various malignant tumors such as PPB, rhabdomyosarcoma, cystic nephroma, and thyroid tumors. These related malignancies are collectively referred to as DICER1 syndrome [12]. A potential for progression from CPAM to PPB has been reported [4, 13, 14] and the mutation of DICER1 gene is speculated to be associated with malignant transformation, although no mechanisms have been elucidated [15, 16]. Mutations in DICER1 gene have been confirmed in approximately 60% of PPB patients and the presence or absence of mutations may not affect differences in PPB disease type or survival rate [3]. However, careful follow-up is required because the patient has the mutation in DICER1 gene.


Comments (0)