
Remember me



A 47-year-old woman with a history of smoking was diagnosed with PLCH through a transbronchial lung biopsy. Despite smoking cessation, cystic changes in the lungs progressed, and the patient developed pneumothorax and central diabetes insipidus owing to the extrapulmonary involvement of PLCH, which required desmopressin. At the age of 36 years, the patient was referred to our hospital for lung transplant evaluation; however, it was deemed premature for transplantation given her stable respiratory status and preserved exercise tolerance at that time. Subsequently, the patient's condition gradually deteriorated. She experienced repeated pneumothorax and became oxygen inhalation dependent at the age of 39 years. The patient refused a second lung transplant evaluation because of financial problems; therefore, conservative treatment was continued for several years.
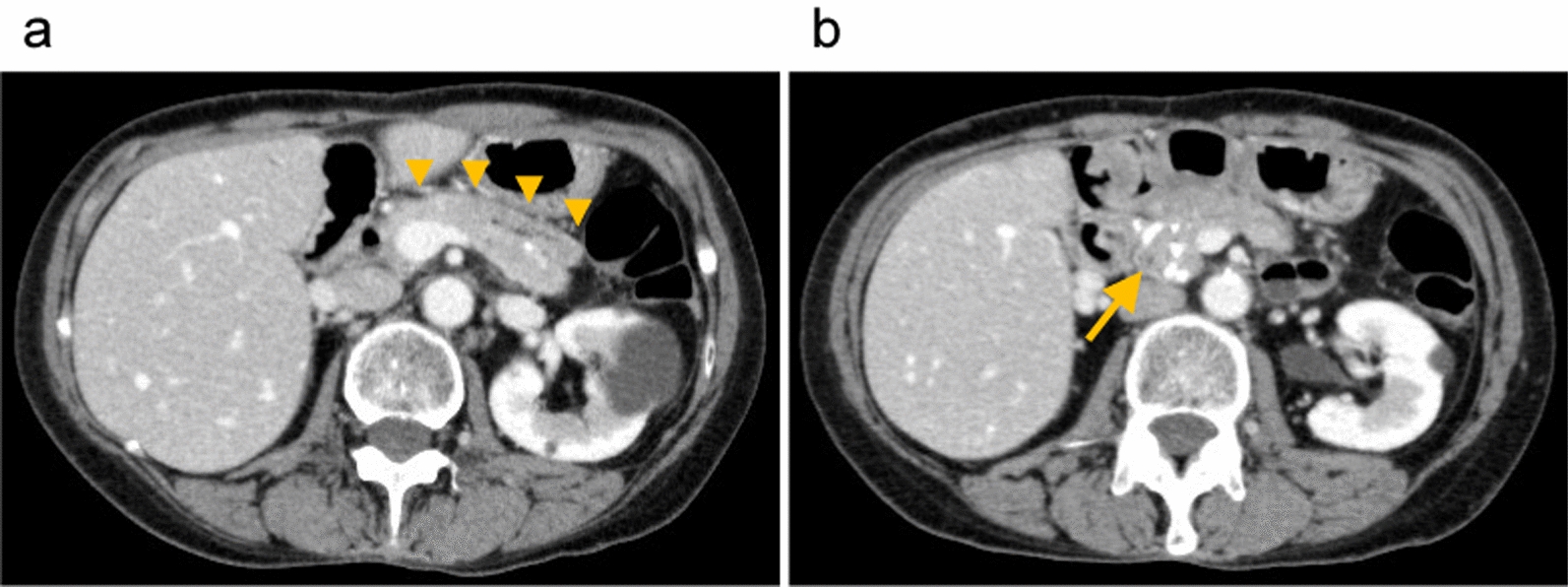
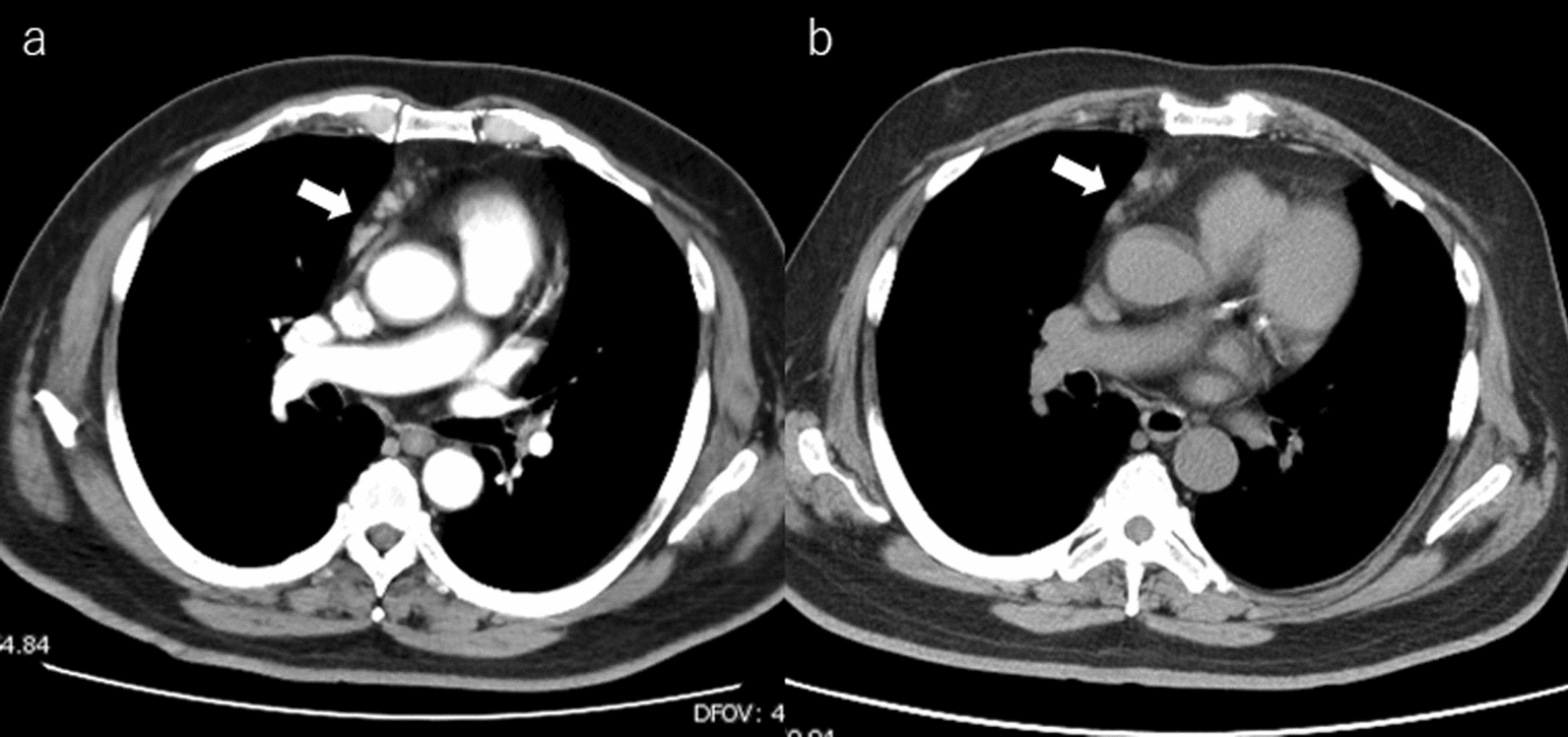
At the age of 47, the patient rapidly developed leg edema and exertional dyspnea. She was referred to a local hospital, and ultrasonic cardiography suggested PH. Her respiratory status did not improve despite diuretic therapy. Consequently, she was admitted to our hospital because of severe respiratory failure. The peripheral oxygen saturation was 92% with 10 L/min oxygen inhalation. Chest radiography revealed bilateral reticular opacities and enlarged pulmonary arterial shadows. Contrast-enhanced computed tomography (CT) revealed numerous thin- and thick-walled pulmonary cysts, as well as large thrombi extending from the pulmonary trunk to both the main pulmonary arteries without deep venous thrombosis and peripheral pulmonary artery thrombosis (Fig. 1A–C). Right heart catheterization revealed PH with a mean pulmonary artery pressure of 48 mmHg. The patient was treated with riociguat and macitentan for PH along with systemic anticoagulation with warfarin. The prothrombin time-international normalized ratio (PT-INR) was maintained between 2.5 and 3.0. After 3 months of anticoagulation therapy, the thrombi disappeared from the pulmonary trunk and were limited to both main pulmonary arteries on CT (Fig. 1D). However, the patient remained bedridden owing to severe exertional dyspnea and was easily desaturated even under nasal high-flow oxygen therapy. The patient was evaluated and deemed a candidate for LT. However, it was difficult to wait for deceased-donor LT, therefore we decided to perform LDLLT. Her brother and daughter were suitable donors, and the right lower lobe of her brother and the left lower lobe of her daughter were estimated to provide 77% of the recipient’s predicted forced vital capacity.
Fig. 1
Radiological images. A Bilateral enlarged pulmonary artery shadows are seen in the chest radiograph. B The computed tomography shows numerous thin-walled pulmonary cysts. C Massive thrombi in dilated pulmonary artery extending from the pulmonary trunk to both main pulmonary arteries are revealed at initial enhanced computed tomography. D Follow-up computed tomography after 3 months of anticoagulation therapy reveals markedly shrinking thrombi limited in the main pulmonary artery wall
OperationThe surgery was performed through a clamshell incision. Central extracorporeal membrane oxygenation (ECMO) was established via arterial cannulation of the ascending aorta and venous cannulation from the right atrium to the superior vena cava and right femoral vein. The right lung was removed using staplers for vascular and bronchial division. The right main pulmonary artery was encircled between the superior vena cava and the ascending aorta for subsequent clamping at the proximal of the thrombi. The donor’s right lower lobe was implanted, and the graft’s lower bronchus and pulmonary vein were anastomosed to the main bronchus and left superior pulmonary vein of the recipient, respectively. The right main pulmonary artery was clamped between the superior vena cava and the ascending aorta. The remaining thrombi in the right main pulmonary artery were removed (Fig. 2A). To deal with the size mismatch between the dilated recipient’s right main pulmonary artery and the lobar pulmonary artery of the graft, the recipient’s pulmonary artery was wedge-excised and plicated. Anastomosis of the pulmonary arteries was conducted in an end-to-end fashion (Fig. 2B), and the right lung was reventilated and reperfused. The left lower lobe of the patient’s daughter was transplanted using a similar technique. The ECMO was smoothly weaned off, and the ECMO circuit was removed. The PaO2 on admission to the intensive care unit was 498 mmHg with 100% oxygen inhalation.
Fig. 2
Intraoperative findings. A Thrombi (arrow) were observed inside the opened right main pulmonary arteries. B The pulmonary artery of the graft (asterisk) was anastomosed to the dilated main pulmonary artery of the recipient, the size of which was reduced with direct plication (arrowheads). C The schema of A. D The schema of Fig. 2B. SVC: superior vena cava, PA: pulmonary artery, RA: right atrium
Postoperative courseAnticoagulation therapy with heparin (10,000 U/day) was initiated on postoperative day two. Epidural anesthesia was not used because of the need for anticoagulation therapy. One week after transplantation, acute rejection was suspected and steroid pulse therapy was administered. A human leukocyte antigen (HLA) antibody test was concurrently performed and revealed positivity for donor-specific antibodies against HLA class II antigens in her daughter. The patient was diagnosed with antibody-mediated rejection and treated with plasmapheresis for 5 days followed by intravenous immunoglobulin therapy for 3 days. Subsequently, anti-thymocyte globulin therapy was also given for 5 days considering the prolongation of clinical symptoms, and the patient’s respiratory status gradually improved following treatment. A CT scan conducted 1 month after the operation showed no residual thrombi in the pulmonary arteries. Consequently, the anticoagulation therapy was switched to warfarin, with the PT-INR maintained between 1.5 and 2.5, as required for the treatment of pulmonary arterial hypertension and chronic thromboembolic pulmonary hypertension. The patient was discharged on postoperative day 64 without any oxygen requirement. At the two-year follow-up, she was doing well and was leading a normal life.
Comments (0)