In Japan, only 1.8% of lung cancer surgery patients undergo pneumonectomy, making it a relatively uncommon procedure [1]. However, it is important to note that the quality of life of these patients can deteriorate due to complications such as chest pain, arrhythmia, and dyspnea. Bronchial obstruction after post-pneumonectomy remains a rare phenomenon, and there is a paucity of literature addressing this issue [2]. After unilateral lung removal, absorption of thoracic air leads to mediastinal parenchymal shift. The main bronchus and bronchus intermedius were compressed by the pulmonary artery and vertebra. The lack of recent pneumonectomy cases has limited pulmonologists’ exposure to these scenarios. Therefore, this report serves as a valuable reminder of the possibility of bronchial obstruction after pneumonectomy.
The critical condition of the patient warrants preparation of an ECMO system. While this decision may seem controversial, given the obvious need for curative thoracotomy, “stand-by” ECMO was considered essential in this precarious situation based on the patient’s condition and the experience of the medical team.
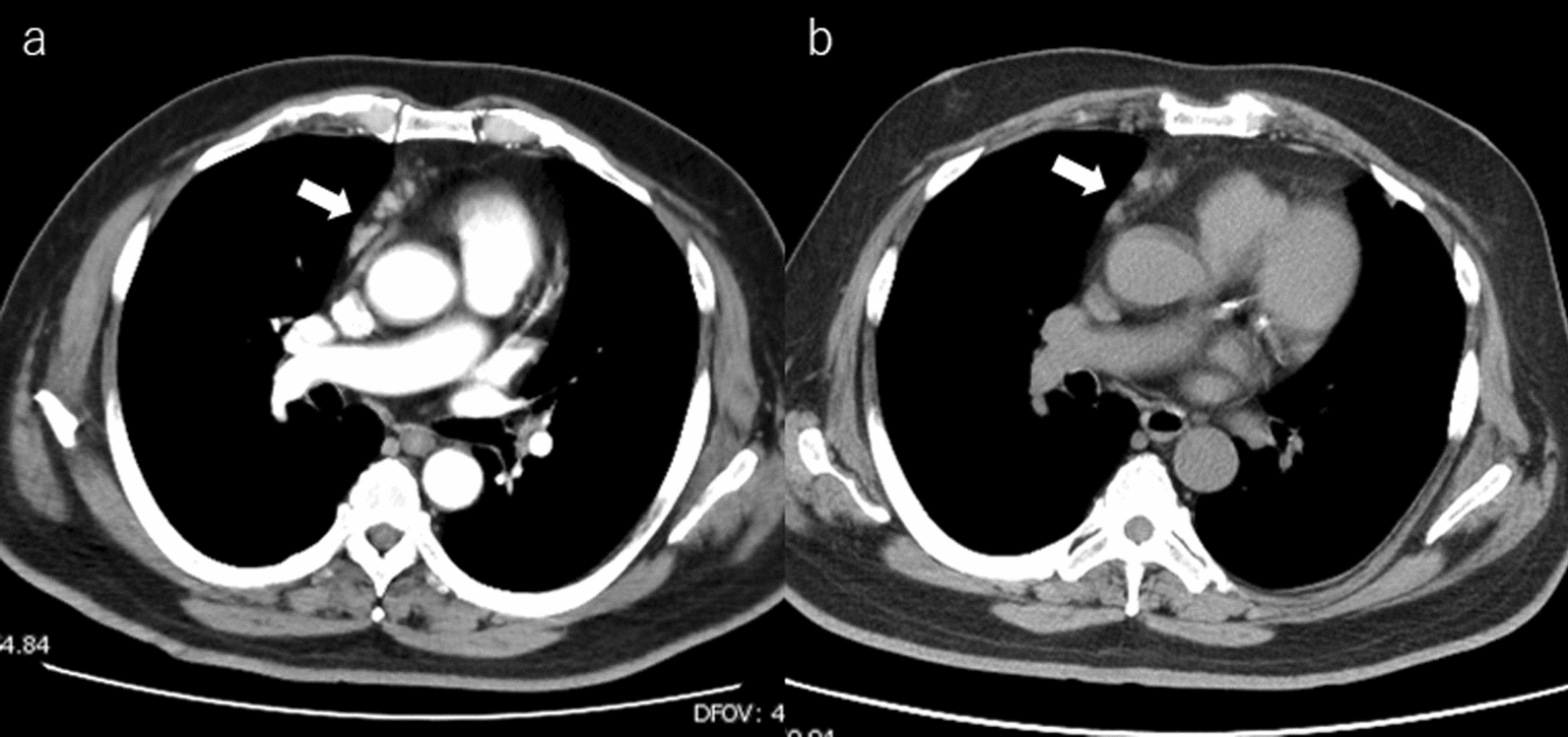
We opted for an 8 cm skin incision and meticulously dissected the chest wall layer by layer using fine scissors, specifically ‘Metzenbaum scissors’, with utmost care to avoid cardiac injury. CT showed minimal space between the pericardial wall and pleura, and direct attachment between the two structures appeared rare after several months to years of history of mediastinal shift.
Previous studies have reported several articles on the treatment of PPS, including tissue expander implantation [3,4,5,6], gas injection [7, 8] and stenting [9]. Unfortunately, tissue expanders for thoracic cavity stabilization are not approved for use in Japan due to insurance regulations, which limits their availability for emergency surgery. In addition, stenting for benign bronchial obstruction is not formally approved in Japan, and the procedure is risky in patients with severe pulmonary conditions. In this case, we employed SF6 gas, which is a readily available and straightforward procedure. SF6 exhibits twofold expansion within 72–92 h post-injection, subsequently returning to the injected volume within a week [10]. Kimura reported that this patient complained of chest discomfort 3 days after the injection [11]. Nevertheless, to alleviate any chest discomfort arising from gas expansion, 400 mL of SF6 was administered under radiographic guidance. It is particularly crucial to administer a conservative amount of SF6 into the thoracic cavity during initial administration, anticipating its volume will double in a few days. For subsequent thoracic administrations, the amount administered initially should serve as a reference. It is advisable to carefully elicit feedback from the patient regarding thoracic symptoms experienced in the days following the thoracic administration. As reported by previous investigators, the interval between infusions increases with each subsequent injection. The exact mechanism underlying this phenomenon remains elusive, but it is hypothesized that thickening of the intrapleural wall retards SF6 absorption. Indeed, our experience supports this, as we were able to extend the infusion interval from 2 months to more than 11 months, coinciding with gradual intrapleural wall thickening and fluid collection. It is known that C3F8 is also adapted gas for an ocular injection in ophthalmic surgery which is absorbed more slowly than SF6 and remains the thoracic cavity for a long duration. To prevent incidents due to mix-ups, our department of ophthalmology has chosen to exclusively use SF6 and has not adopted C3F8. Although there were plans to purchase and use C3F8 in this case, it became unnecessary due to the stabilization of the thoracic cavity.
Limitations of using SF6 include its status as an off-label application. When explaining to patients, it is necessary to advise against the use of nitrous oxide anesthesia and to avoid high-altitude climbing, air travel and hyperbaric oxygen therapy until the SF6 has dissipated. It is essential to obtain patient consent after discussing the off-label use. Following surgeries for post-pneumonectomy syndrome, water and air are relatively quickly absorbed, hence the use of SF6 would ideally be within 10 day post-operation. Approval from the hospital’s ethics committee is required for off-label uses, therefore, having a system for expedited review is advisable.




Comments (0)