A rearrangement involving one of the NTRK genes, which belongs to the NTRK family, represents a significant oncogenic event in thyroid cancer [12]. The NTRK family includes three genes, NTRK1, NTRK2, and NTRK3, which encode TRKA, B, and C, respectively. Fusions involving the kinase domain of the NTRK gene lead to uncontrolled activation of the tyrosine receptor kinase and, subsequently, the MAPK, PI3K/AKT, and PLC pathways [13]. TRK fusion-positive thyroid carcinoma is more commonly associated with a younger age at diagnosis, and approximately 5–25% of pediatric PTC cases are reported to harbor NTRK gene fusions [10]. In contrast, the reported presence of NTRK fusions in predominantly adult thyroid cancer cohorts is low, ranging from 2.3 to 3.4% [14]. To date, no large-scale study has investigated the incidence of NTRK fusions in Japanese patients with thyroid cancer. As genomic testing has become increasingly common in Japanese clinical practice, the incidence of NTRK fusion in Japanese patients with thyroid cancer is likely to become clear in the near future.
Several NTRK rearrangements have been observed in TCs. Chu et al. investigated 351 primary thyroid cancers, including 186 PTCs, 54 medullary thyroid carcinomas (MTCs), 38 anaplastic thyroid carcinomas (ATCs), 24 Hurthle cell carcinomas (HCCs), 23 follicular thyroid carcinomas (FTCs), 21 poorly differentiated thyroid carcinomas (PDTCs), and five unclassifiable carcinomas [15]. The study reported that NTRK rearrangements were detected in 11 (3.1%) cases, all of which were originally diagnosed with PTC [15]. The observed NTRK rearrangements included ETV6–NTRK3 (n = 4), TPR–NTRK1 (n = 2), RBPMS–NTRK3 (n = 2), SQSTM1–NTRK1 (n = 1), SQSTM1–NTRK3 (n = 1), and EML4–NTRK3 (n = 1) [15]. In another study by Pekova et al., a total of 989 thyroid cancer tissues, including 851 PTCs, 86 MTCs, 19 FTCs, 13 ATCs, 10 PDTCs, 10 HCCs, and 30 borderline thyroid tumor tissues (17 follicular tumors of uncertain malignant potential, 13 non-invasive follicular tumors with papillary-like nuclear features, and 194 benign thyroid tissues) were analyzed [12]. The analyses revealed the NTRK fusion gene in 59 patients with thyroid cancer, 57 of 846 (6.7%) patients with PTC, and 2 of 10 (20.0%) patients with PDTC [12]. In addition, eight types of NTRK fusions were identified: ETV6–NTRK3 (n = 38), TPM3–NTRK1 (n = 5), SQSTM1–NTRK3 (n = 4), EML4–NTRK3 (n = 4), RBPMS–NTRK3 (n = 3), IRF2BP2–NTRK1 (n = 3), SQSTM1–NTRK1 (n = 1), and TPR–NTRK1 (n = 1) [12]. SQSTM1–NTRK1 was also detected in this case. Considering previous reports, the SQSTM1–NTRK1 fusion may be rare.
Larotrectinib was evaluated across 15 tumor types in 159 patients with TRK fusion cancer, and 121 (79%, 95% CI 72–85) of 153 patients had an objective response [16]. Of the 153 patients, 24 (16%) had a complete response, 97 (63%) had a partial response, 19 (12%) had stable disease, and nine (6%) had progressive disease [16]. Furthermore, Waguespack et al. reported the results of pooled data from three phase I/II larotrectinib clinical trials [10]. This study included 29 patients with TRK-fusion-positive thyroid cancer who were treated with larotrectinib. The histology was PTC in 20 (69%) patients, FTC in two (7%), and ATC in seven (24%), and the objective response rate was 71% among 28 evaluable patients [10]. The clinical responses were as follows: 2 (7%) had a complete response, 18 (64%) had a partial response, 4 (14%) had stable disease, and 3 (11%) had progressive disease [10]. The median response was 1.87 months [10]. Treatment-related adverse events (AEs) were reported in 26 patients (90%), the most common being myalgia, fatigue, dizziness, and elevated liver transaminase levels. Most treatment-related AEs were grade 1 or 2 [10]. In our case, the time to response was approximately one month. Furthermore, grade 1 myalgia, which occurred two weeks after the initiation of larotrectinib, was the only adverse effect. Therefore, larotrectinib treatment was effective and treatment-related AEs were tolerable.
To our knowledge, only three case reports of larotrectinib treatment for thyroid cancer have been published. Pitoia reported the case of a PTC patient with ETV6-NTRK3 gene fusion who had previously been treated with sorafenib and lenvatinib [17]. Surprisingly, the patient achieved a durable (sustained for 11 months) complete response after 2 months of larotrectinib treatment and a complete intracranial response in metastatic brain lesions after 7 months of larotrectinib treatment [17]. Saliba et al. reported a case of secretory carcinoma in a patient with ETV6–NTRK3 fusion [18]. Larotrectinib was administered for lung and neck metastases, and a durable response lasting 18 months was achieved [18]. Bargas et al. reported a case of PTC with SQSTM1–NTRK gene fusion [19]. Although the patient had hemoptysis and respiratory distress syndrome with marked dyspnea, all respiratory and thoracic symptoms disappeared two weeks after the initiation of larotrectinib [19]. In addition, the first CT evaluation after 2.5 months confirmed a partial response [19]. Despite our patient's history of mTKI treatment, larotrectinib was effective for distant metastases, similar to two previous case reports of patients with PTC. Therefore, larotrectinib is considered an effective treatment option even for patients with a history of mTKI treatment.
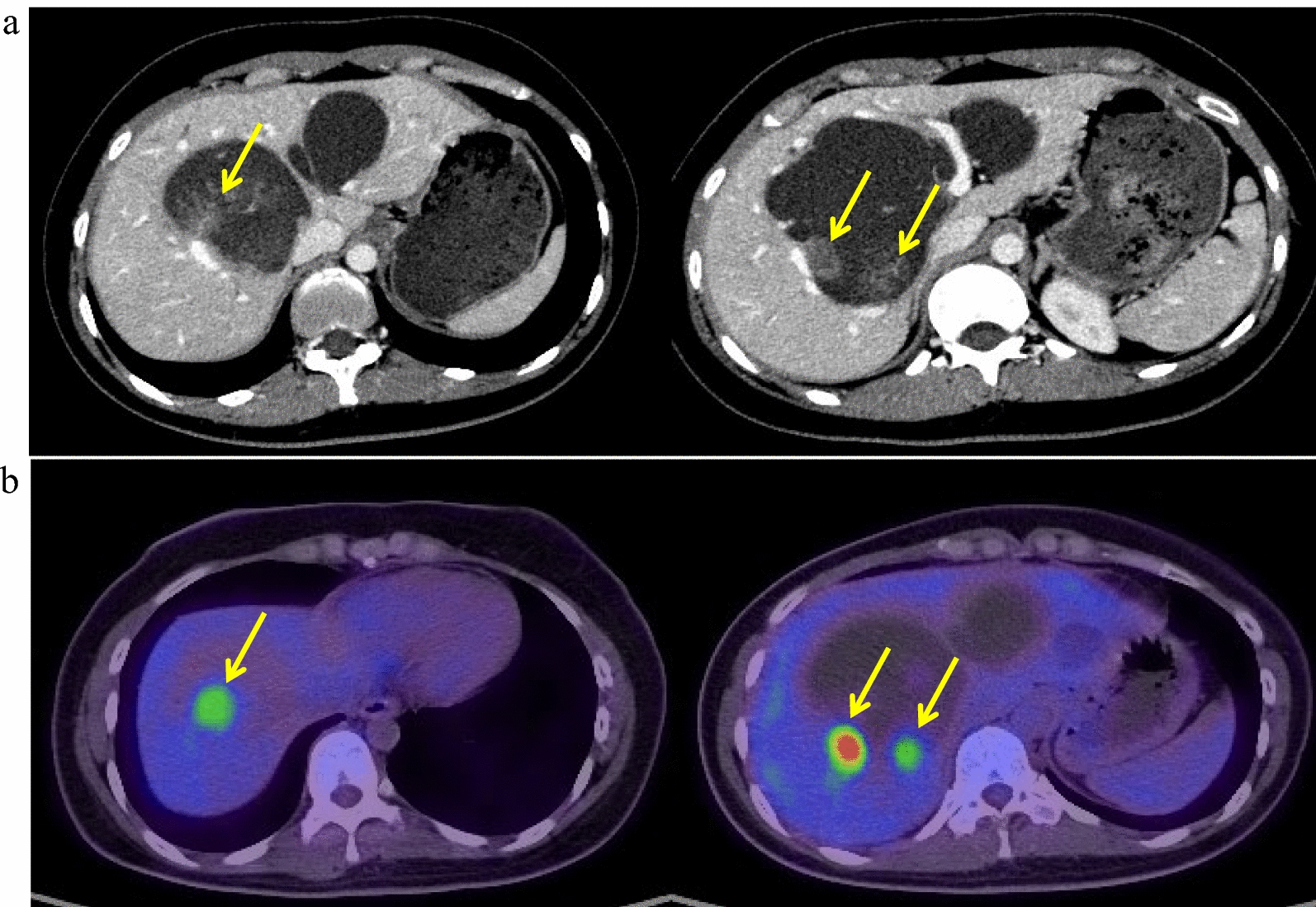
Distant metastases from differentiated thyroid carcinoma (DTC) mainly involve the lungs and bones, and metastases to other sites, such as the liver, are extremely rare [6]. Yoon et al. investigated 38,772 DTC patients and revealed that liver metastasis was observed in only five patients [6]. Although treatment outcomes have not been fully investigated among thyroid cancer patients with liver metastasis, TKIs may be beneficial [20, 21]. In our case, liver metastases were reduced by larotrectinib, which is a good treatment option for patients with TC and liver metastases.
Although the companion diagnostic test for larotrectinib is the FoundationOne CDx (Foundation Medicine Inc., Cambridge, MA, USA), the OncoGuide™ NCC Oncopanel System was performed in our case because the remaining liver biopsy specimens were small. The OncoGuide™ NCC Oncopanel System can generally be performed using fewer specimens than the FoundationOne CDx. In general, it is recommended that a specimen obtained within 3 years be used for genetic testing [22]. In this case, we performed effective genetic testing using fresh specimens.
In our case, the Tg levels decreased immediately after the initiation of larotrectinib. However, the patient was positive for TgAb, which might have affected the Tg levels. In general, an increase or reappearance of TgAb during follow-up is highly suggestive of recurrence or persistence [23]. In contrast, TgAb levels were reported to be correlated with the clinical response to lenvatinib [24]. The mechanism by which the TgAb level was positive after larotrectinib treatment is unknown. However, the TgAb level gradually decreased and liver metastases continued to shrink. Further studies are needed to investigate whether this response is specific to larotrectinib.




Comments (0)