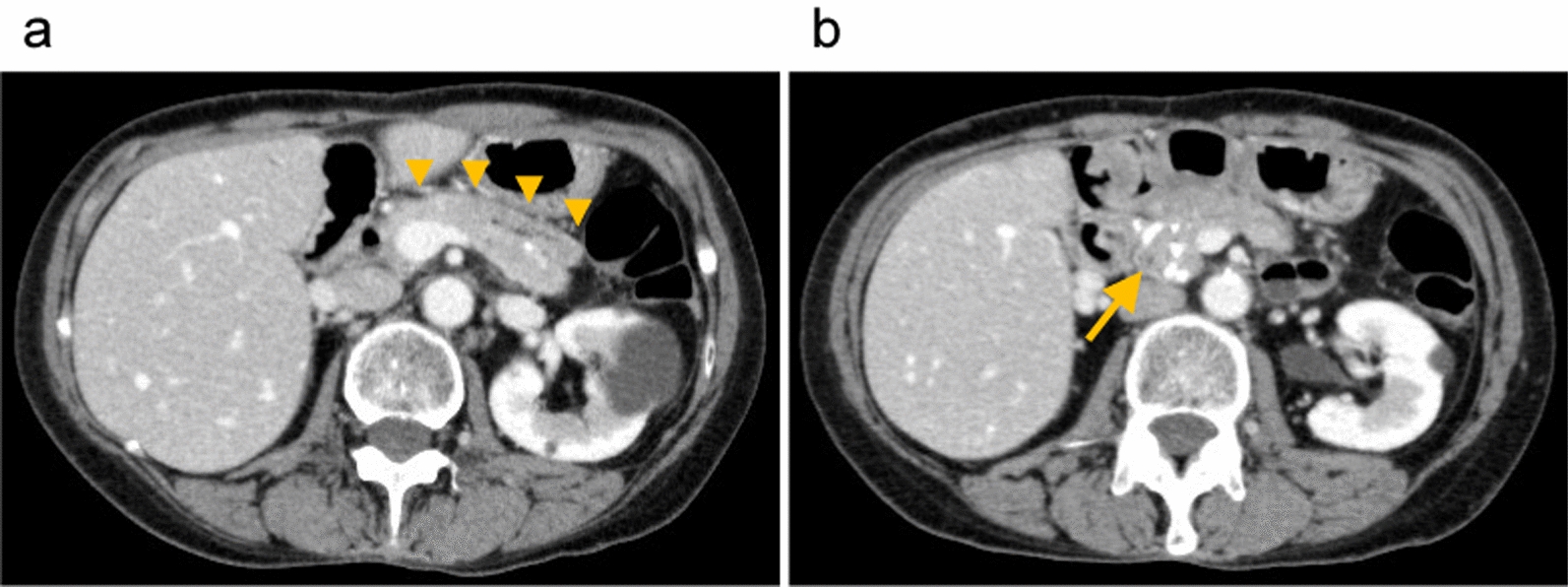
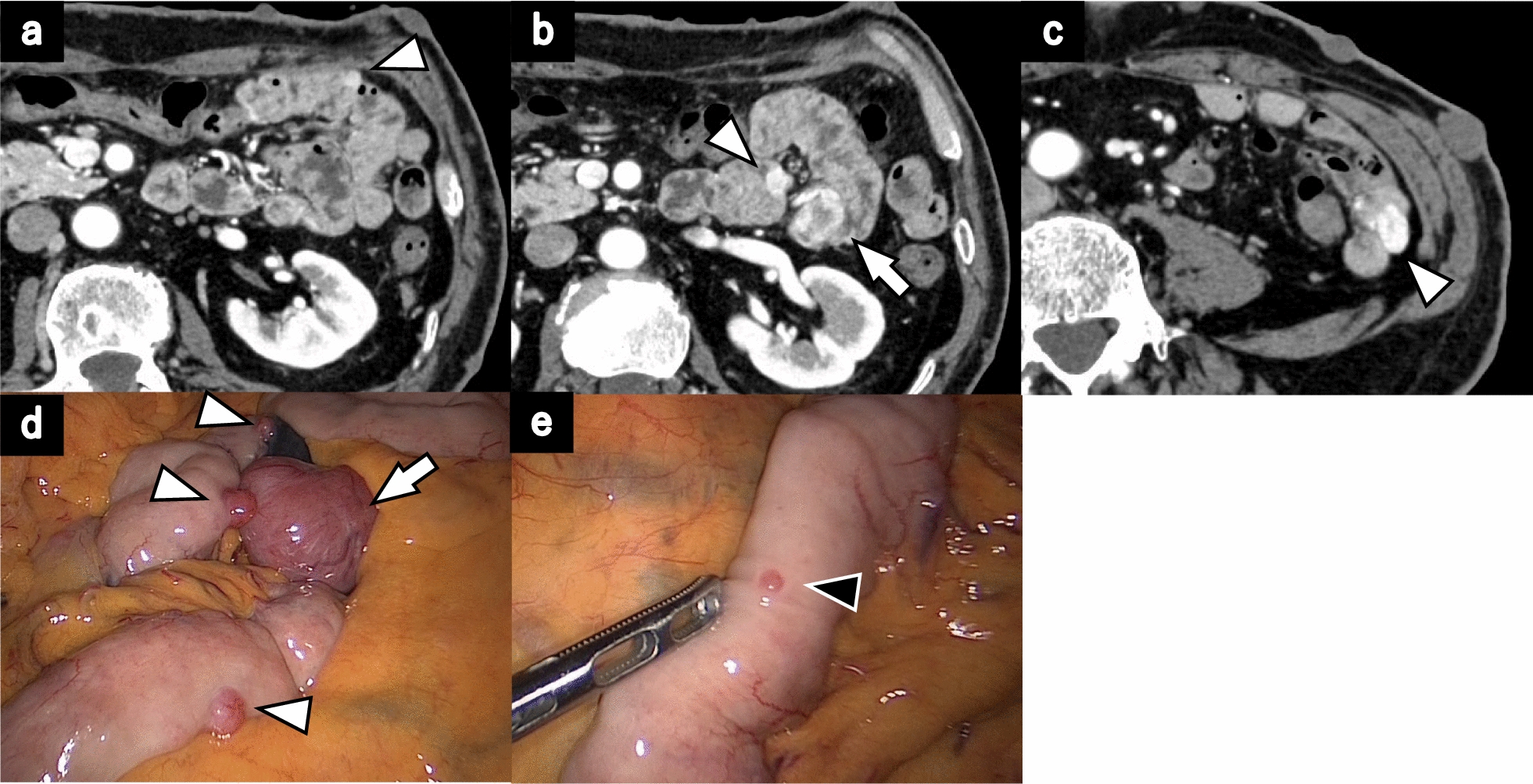
NF1, also recognized as von Recklinghausen disease, is one of the most prevalent autosomal dominant single-gene neurocutaneous disorders [4]. Although patients with NF1 typically present with characteristic skin lesions, gastrointestinal involvement can also occur, with neurofibromas or GISTs being the predominant histologic types [5]. GISTs are the most common gastrointestinal lesions in NF1, with an estimated prevalence of 5%–30% [6]. Although GISTs typically originate in the stomach, GISTs related to NF1 arise in the small intestine in approximately 90% of patients and frequently manifest as multiple lesions [7]. Resectable GISTs with a diameter of 2 cm or more are eligible for surgical resection, which remains the sole curative treatment option. In this case, the presence of anemia requiring blood transfusion led to the decision for early surgical intervention, and lower double-balloon endoscopy was consequently not performed. However, achieving an accurate preoperative diagnosis is important to avoid unnecessary bowel resection.
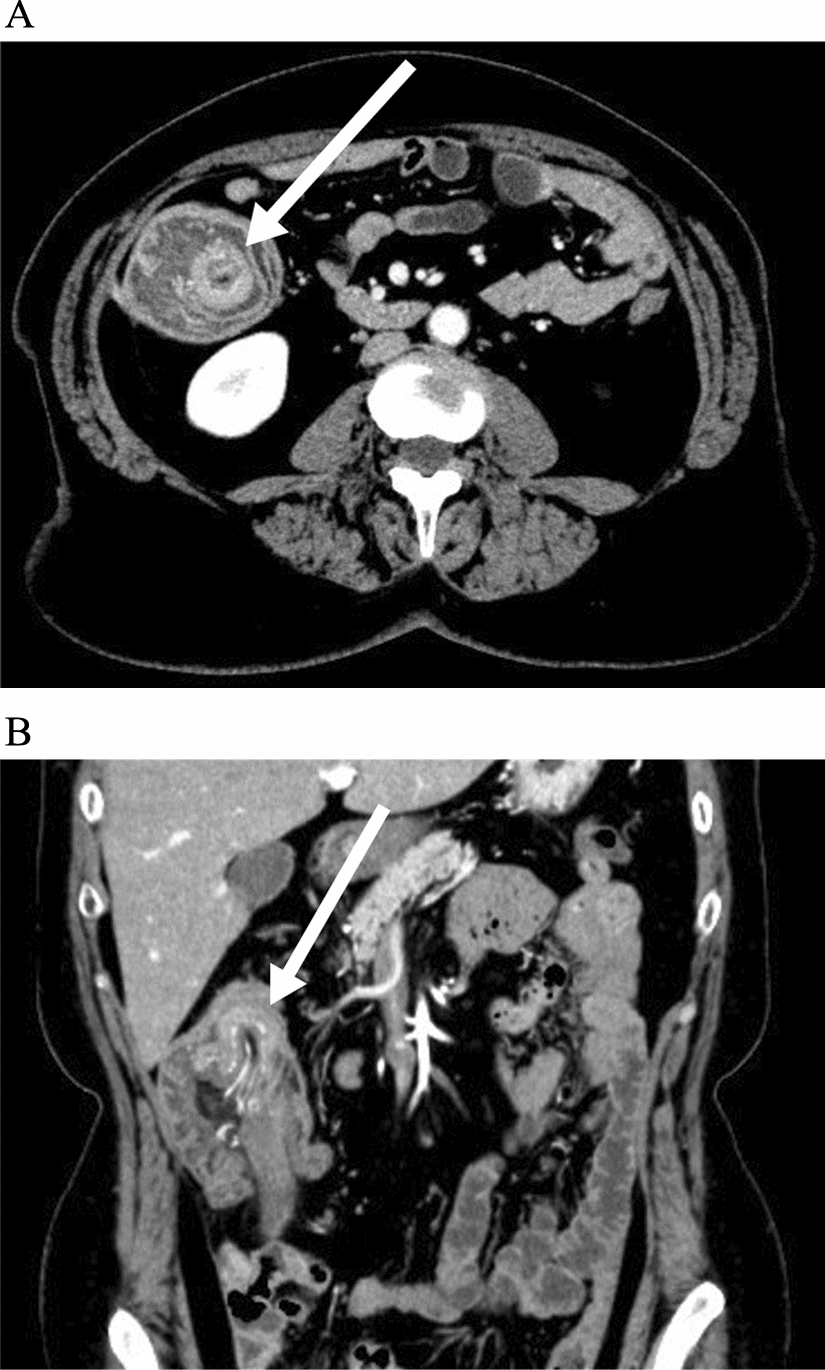
Neurofibromas in the abdomen in patients with NF1 can occur from the esophagus to the rectum, as well as in the peritoneum and mesentery [8]. Lesions are predominantly found in the jejunum, stomach, ileum, duodenum, and colon. These tumors can lead to complications such as obstruction, gastrointestinal bleeding, or perforation. Neurofibromas in the appendix are extremely rare, with only ten patients documented to date [9,10,11,12,13,14,15,16,17,18]. Among these patients, seven presented with abdominal pain, while only two remained asymptomatic, similar to our study patient. The most common preoperative diagnosis was appendicitis in six patients. Notably, only one case report has documented a preoperative diagnosis of neurofibroma, indicating the difficulty in establishing an accurate preoperative diagnosis. Furthermore, no case report has documented the development of other tumors in the digestive tract, as observed in our patient.
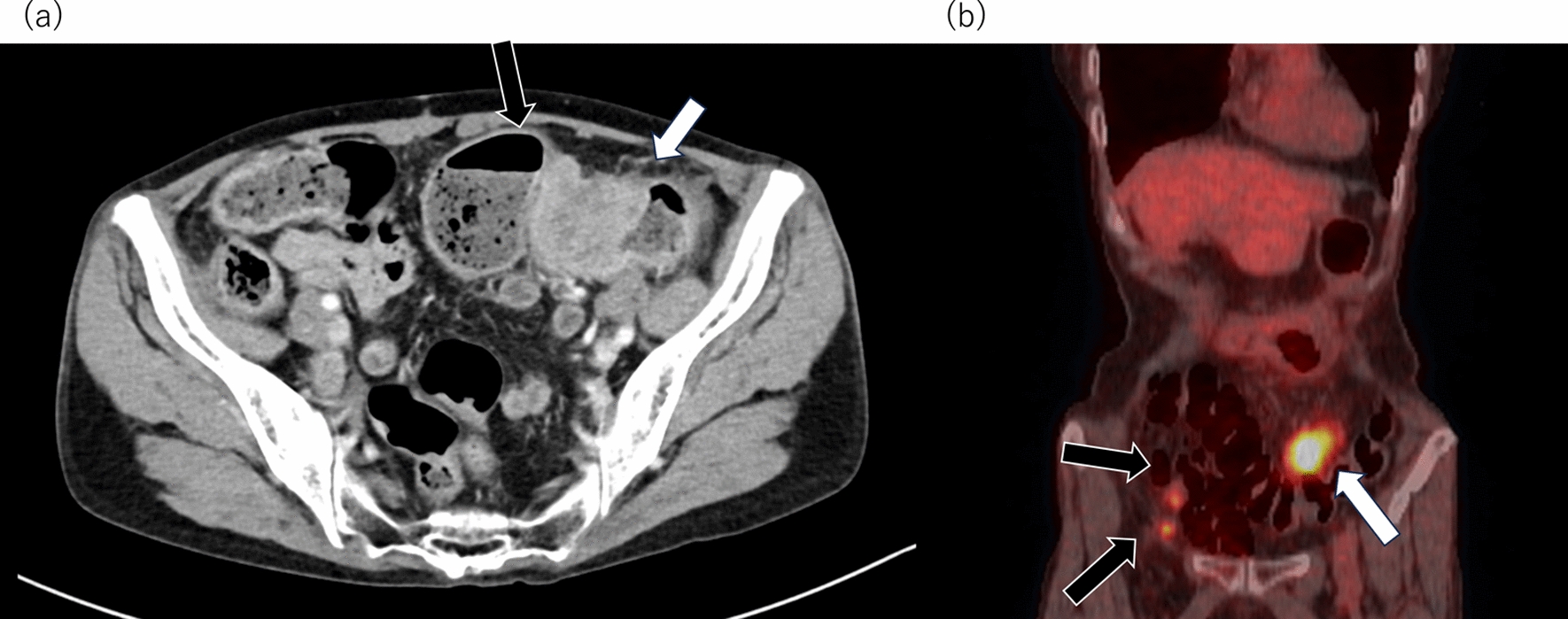
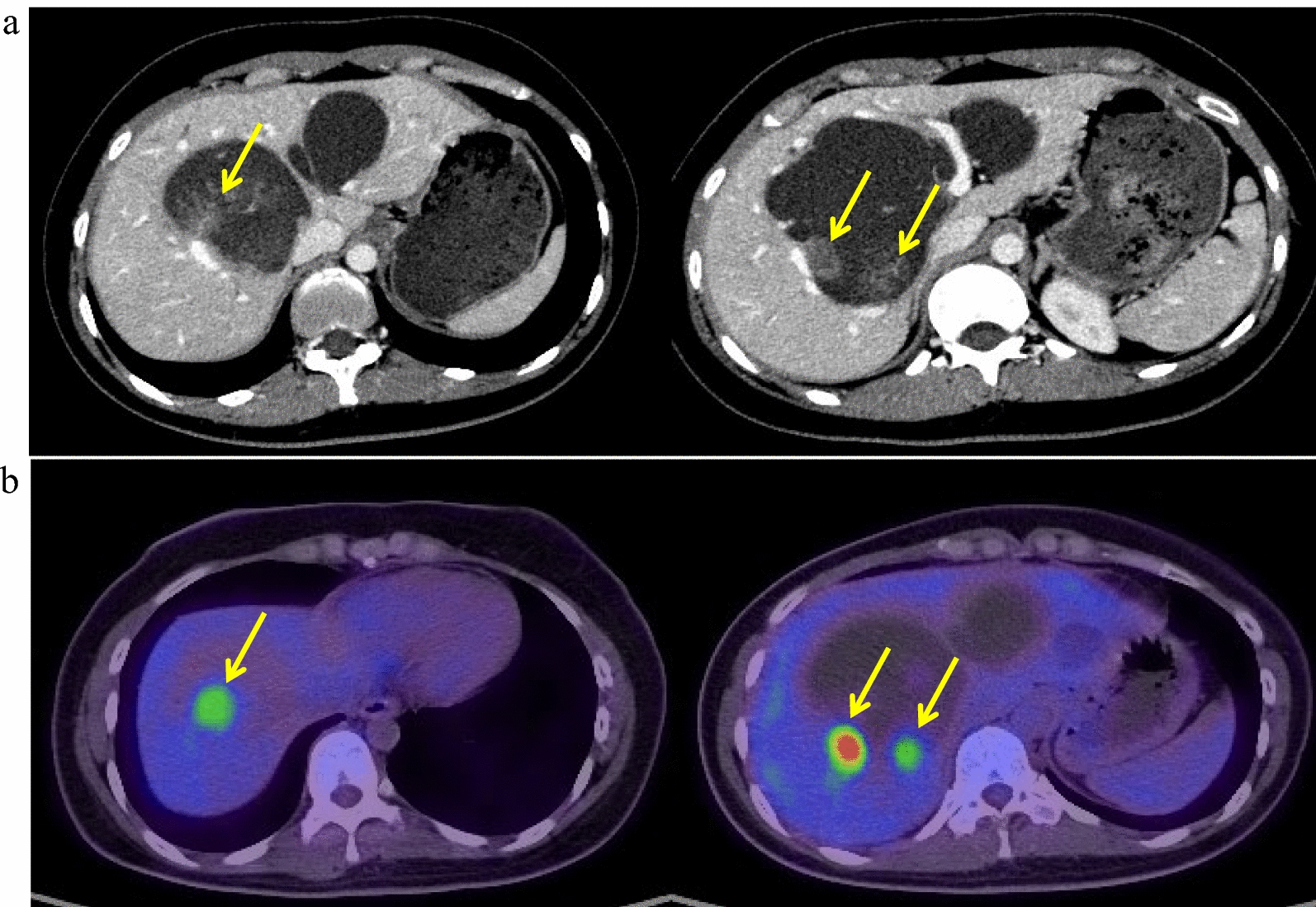
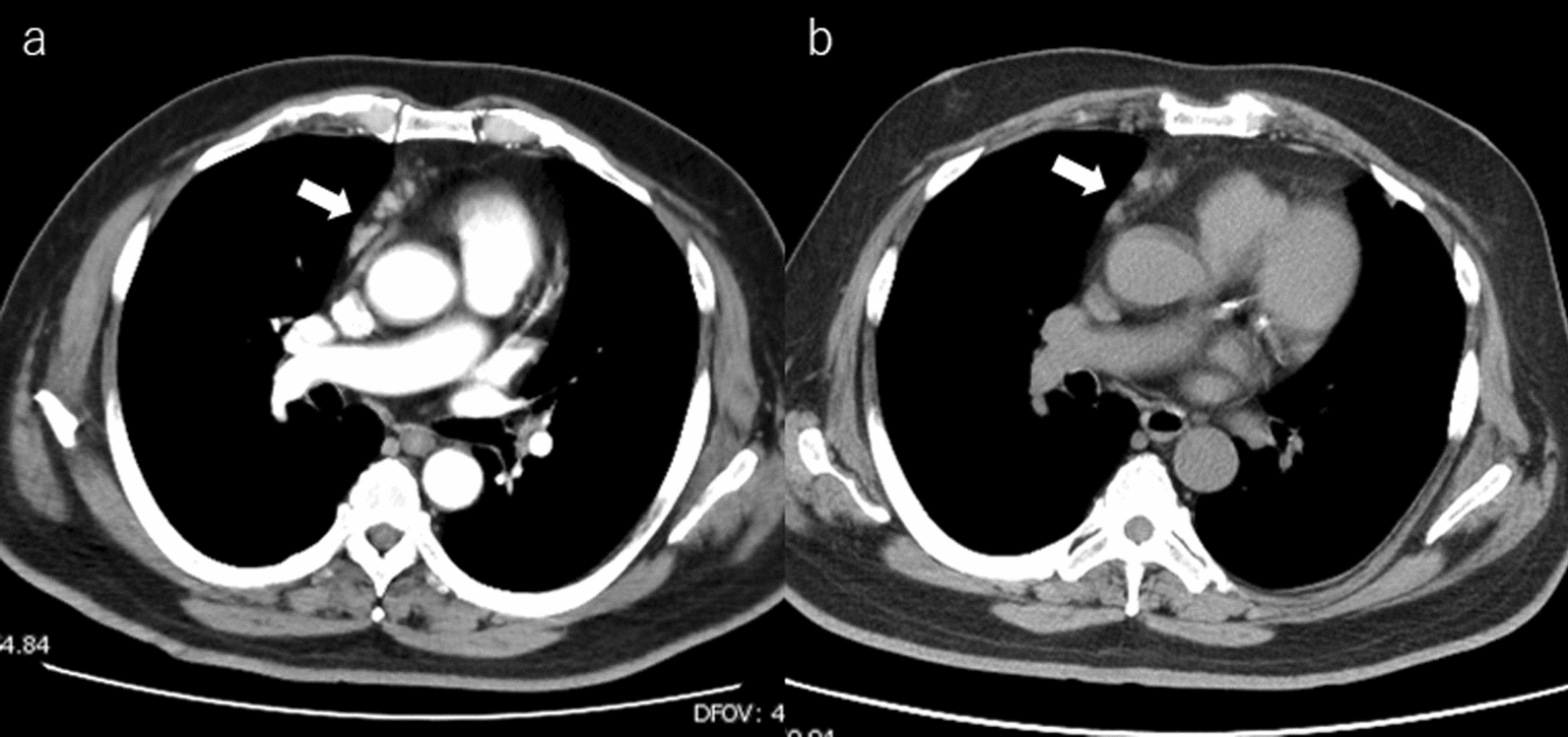
The preoperative diagnosis of appendiceal tumors in patients with NF1 is often challenging. Neurofibroma, which can occur at any site, should be considered as a potential differential diagnosis. However, in previous reports, preoperative diagnosis was not accurately made in most cases, underscoring the difficulty of making a precise preoperative diagnosis. Moreover, distinguishing between benign and malignant lesions can be challenging. Although neurofibromas are benign tumors, patients with NF1 are at increased risk of various types of malignancies [19]. Patients with NF1 have an 8–12% risk of developing malignant peripheral nerve sheath tumors [20]. Therefore, the possibility of malignancy should always be considered when evaluating gastrointestinal lesions in patients with NF1. In our patient, FDG accumulation was observed on PET/CT. It is already known that GIST shows uptake on PET/CT, and the preoperative imaging findings in this case were also consistent with GIST [21]. In patients with NF1, there have been reports indicating that FDG uptake is observed to some extent in superficial lesions, and the degree of FDG uptake is useful for identifying malignant lesions [22]. However, there are no significant reports regarding gastrointestinal lesions in NF1 patients, and no mention of PET findings in case reports of appendiceal neurofibroma. On the other hand, previous reports have documented cases presenting with inflammation, making it difficult to completely rule out the possibility that FDG uptake in this case could be related to some form of inflammation occurring during the clinical course. Therefore, the interpretation of the results should be done with caution, and further case accumulation is necessary in the future (see Table 1).
Table 1 Previous case reports of appendiceal neurofibroma in a patient with von Recklinghausen’s diseaseSurgical resection is the standard of care for appendiceal neurofibroma. This treatment is aimed at improving symptoms, preventing complications, and avoiding malignant transformation [5]. Komo et al. performed a cecectomy to ensure negative surgical margins for an intraoperatively diagnosed appendiceal mass [11]. They stated that if the postoperative pathologic diagnosis had been appendiceal cancer or low-grade appendiceal mucinous neoplasm with positive margins, a secondary ileocecal resection with or without lymph node dissection would have been necessary. In this case, considering the possibility of malignant infiltration, laparoscopic ileocecal resection with lymph node dissection was performed. However, no consensus exists regarding appropriate surgical procedures including the necessity of performing lymph node dissection.
Patients with NF1 may present with multiple comorbidities that require careful monitoring. Patients with NF1 are approximately 2.7 times more likely to develop malignancies than the general population, highlighting the necessity for meticulous follow-up [23]. In addition, lesions exhibiting growth or associated with pain may indicate malignancy and warrant frequent evaluation [24]. The appendiceal neurofibroma was discovered incidentally in an asymptomatic patient during postoperative follow-up for GIST. This finding suggests that even asymptomatic patients may be at risk for developing additional lesions, indicating that heightened surveillance could be beneficial.




Comments (0)