Here, we describe the case of a patient with multiple foci of RDD in the cecum and sigmoid colon. RDD is a rare non-Langerhans cell histiocytosis first reported in 1965 by Destombes [6]. Later, Rosai and Dorfman summarized 34 cases and coined the term sinus histiocytosis with massive lymphadenopathy, which was later changed to RDD [6]. Histologically, the hallmark of RDD is the presence of variable numbers of intact lymphocytes within the histiocytic cytoplasm, a phenomenon referred to as lymphocytophagocytosis or emperipolesis, which is defined as lymphocytic penetration of and movement into the histiocyte [4]. Immunohistochemical studies are widely accepted for diagnosis, and the typical histiocytic markers used for diagnosis demonstrate positivity for S100, fascin, and/or CD68 [3]. Reactive inflammatory processes such as immune deficiency and viral infection have also been suggested to play a role in the pathogenesis of RDD, although no definitive evidence to support any etiology has been found [7].
Classic RDD presents with massive bilateral painless cervical lymphadenopathy with associated fever, weight loss, and night sweats [8]. Most patients with RDD with nodal involvement present with cervical, mediastinal, axillary, and inguinal nodes [9]. However, our patient was asymptomatic, had no massive lymphadenopathy, and had an extranodal lesion in the colon. The main lesion originated from the colon, and the lymph nodes which was included in the resected specimen also contained RDD. It has been reported that 43% of patients with RDD present with extranodal involvement, including the skin, soft tissues, upper and lower respiratory tract, bone, oral cavity, and genitourinary tract [3, 5, 9]. However, RDD involving the colon is a rare condition. A search of the PubMed database using the keywords “Rosai–Dorfman disease” and “colon” for articles published from 1981 to December 2023 and related articles identified 21 cases of RDD of the colon in 13 articles, including the current case [2, 7, 10,11,12,13,14,15,16,17,18,19,20]. Owing to the paucity of information, it was difficult to discuss the actual cause of the occurrence and progression, of RDD from the 21 previously reported cases. However, we speculated that one of the possible causes of this case might be the long-term chemotherapy that our patient underwent for lung cancer. Shukla et al. reported a case of relapse after treatment for Hodgkin disease. Recurrent lesions in the cervical lymph nodes and bone marrow responded well to chemotherapy. However, only the ileocecal mass was ineffective and resected, and a diagnosis of RDD was made [13]. Although a report of only 2 cases does not indicate an increased risk of developing RDD after chemotherapy, other neoplastic lesions, including RDD, might be considered if the recurrent lesions do not respond to treatment as expected or if they recur atypically.
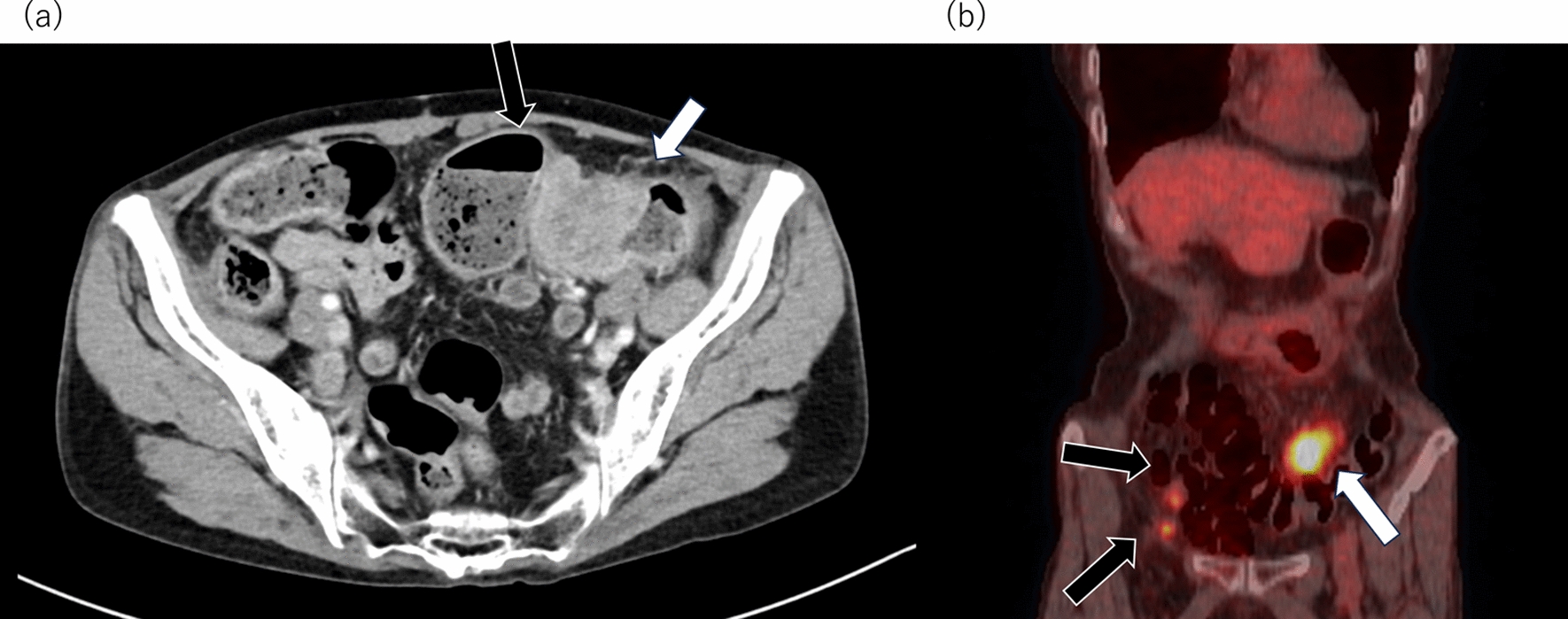
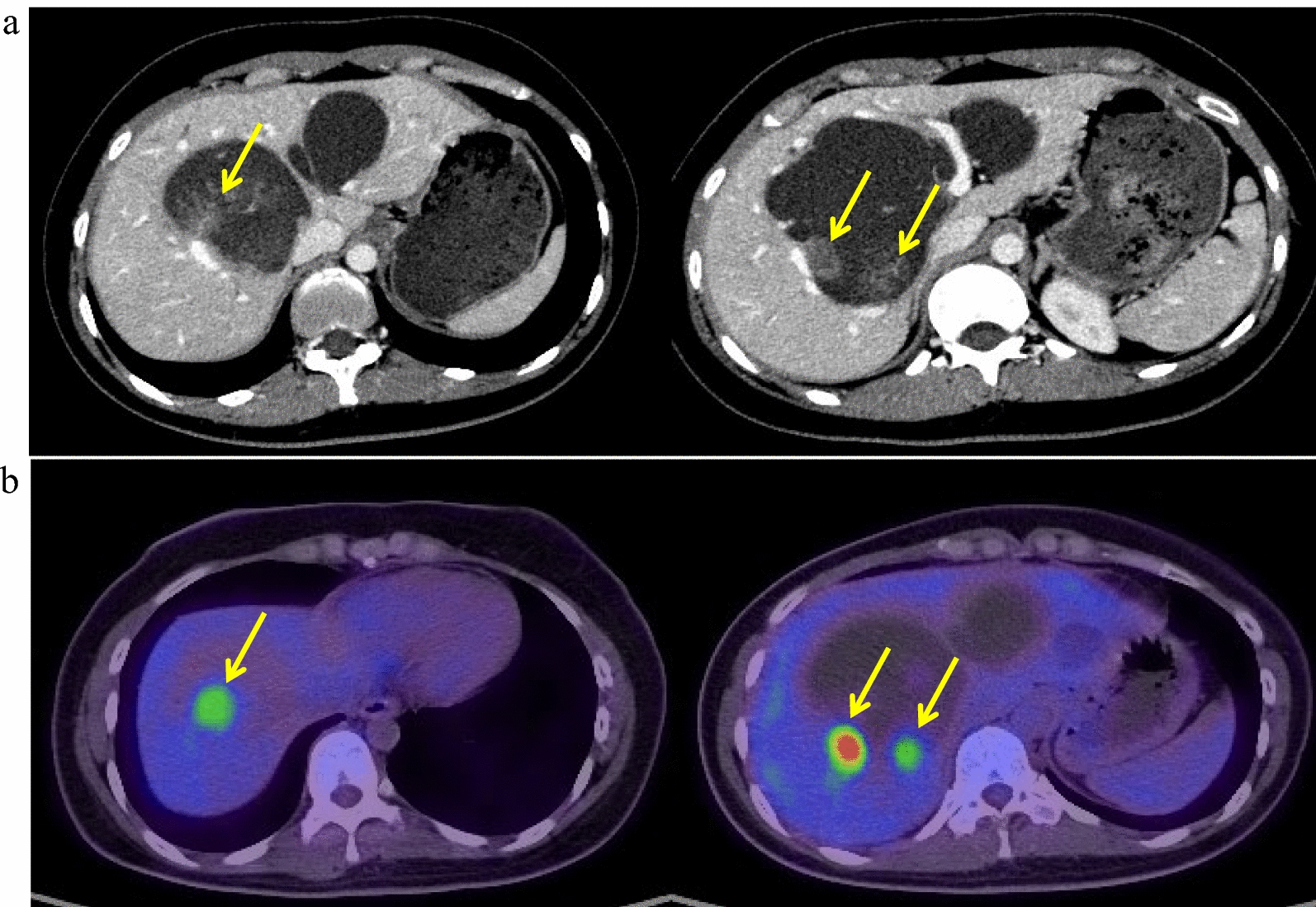
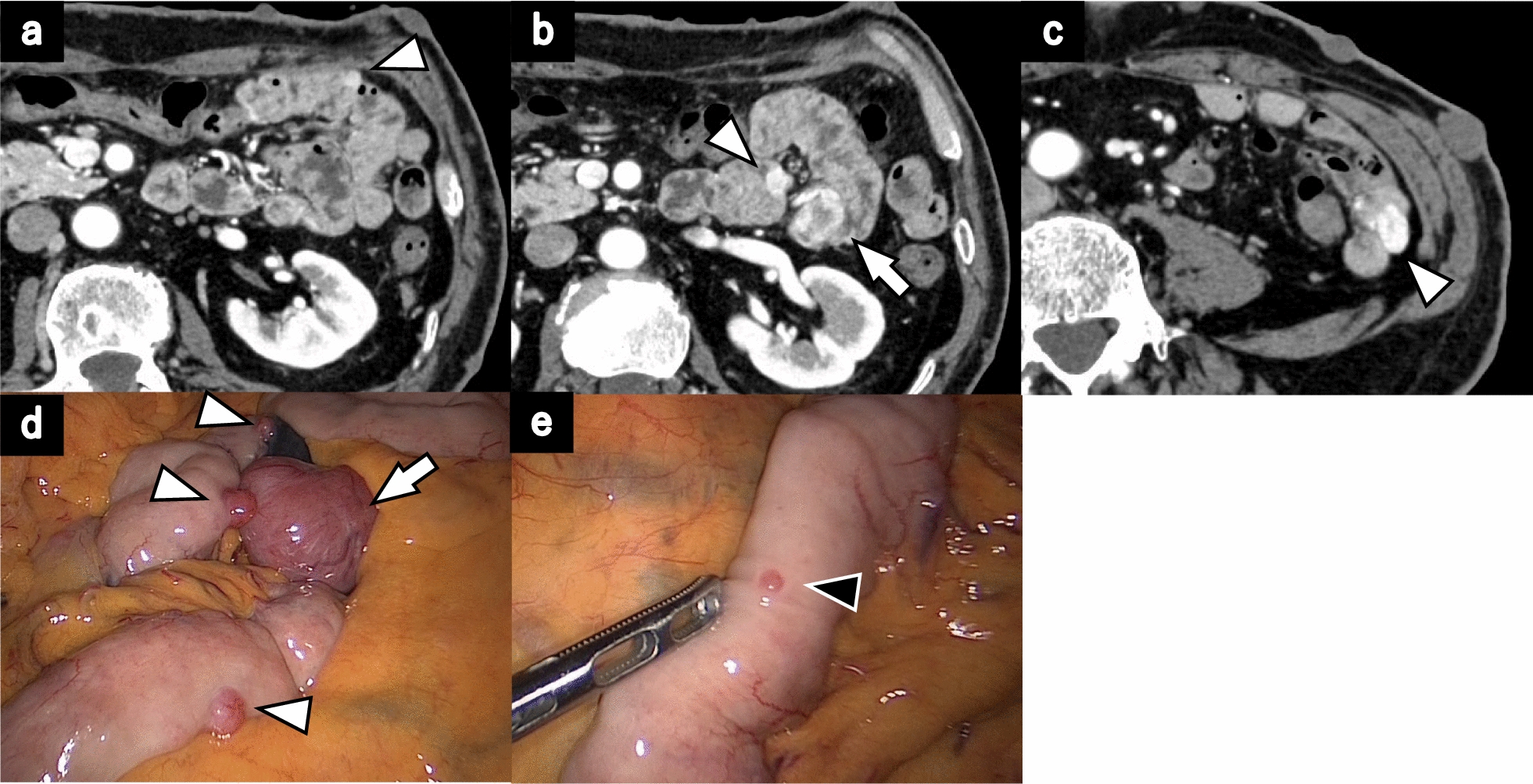
A definite diagnosis of RDD in some organs cannot always be made before surgery because sufficient tissue specimens cannot be obtained. No standard therapy has been established for RDD treatment. However, surgical resection might be helpful for both the diagnosis and treatment, while minimally invasive surgery would be helpful. Among the previous cases, none of these reports described multiple RDD involving the colon treated with minimally invasive surgery, and no reports of laparoscopic surgery for primary RDD of the colon other than our case. In our case, rapid intraoperative histology was performed for both colonic lesions after the resection. However, it was still difficult to make a definitive diagnosis. Even if no malignant findings were found by rapid intraoperative histology, PET-CT still showed the uptake of fluorodeoxyglucose in both lesions, and malignancy was initially suspected. Thus, surgical resection was considered to be necessary.
In one case, multiple tumors occurred simultaneously in the colon, as in this case [20]. As mentioned in the Introduction, primary RDD of the gastrointestinal tract is rare, and classic RDD is characterized by bilateral lymphadenopathy [8]. Therefore, multiple lesions may be uncommon in RDD.
Regarding the prognosis of RDD, recurrence was observed in 2 of the previous 21 cases [14, 15], 1 of which died due to recurrence [15]. Due to the small number of previous cases of RDD originating from the colon, it would be difficult to determine the pattern of recurrence or recurrence rate. However, regular follow-up should be considered even after complete resection.




Comments (0)