
Remember me


Overall, 793 participants were enrolled into PUNCH CD3-OLS, 697 participants received RBL (safety population), and 676 completed at least 8 weeks of study follow-up (mITT population). Within the safety and mITT populations, 90 participants had medical record documentation of IBS, which included participants taking IBS-related concomitant medications. Baseline characteristics in participants with and without IBS were generally comparable, although the median (range) age was lower in the IBS subgroup [57 years (43, 69)] than in the non-IBS subgroup [65 years (50, 74)] (Table 1). Likewise, participants with IBS were more likely to have a history of anxiety and depression (63.3% and 53.3%, respectively) than participants without IBS (36.7% and 34.9%, respectively). Most participants with and without IBS were female (76.7% vs. 68.9%, respectively) and White (95.6% vs. 93.6%, respectively). At the time of RBL administration, 13 participants with IBS (14%) were taking IBS medications, with most (n = 9) taking loperamide (Supplementary Table 2).
Table 1 Participant demographics and baseline characteristics (safety population)A total of 32.2% of participants with IBS and 25.9% of participants without IBS received RBL for their first CDI recurrence (i.e., second CDI episode); 41.1% of participants with IBS and 33.3% without IBS had experienced ≥ 4 prior episodes (Table 1). In the IBS subgroup, participants predominantly had a medical history of abdominal pain (11.1%), nausea (12.2%), and constipation (18.9%). In participants without IBS, the corresponding proportions were 7.6%, 7.9%, and 9.4%.
SafetyThrough 8 weeks after RBL administration, 57.8% (52/90) and 45.8% (278/607) of participants with and without IBS had a TEAE, respectively (Table 2). In both the with IBS and without IBS subgroups, most participants had TEAEs of mild (22.2% and 20.1%, respectively) or moderate (26.7% and 18.8%, respectively) severity. Between 8 weeks and 6 months of follow-up, 26.7% (24/90) of participants with IBS and 22.4% (136/607) of participants without IBS had a TEAE. The most common TEAEs in both subgroups were gastrointestinal disorders, reported in 40.0% (36/90) and 27.8% (169/607) of participants with and without IBS through 8 weeks, respectively, including diarrhea (16.7% and 11.5%, respectively), abdominal pain (16.7% and 9.1%, respectively), and nausea (6.7% and 5.8%, respectively) (Table 3). Gastrointestinal disorders remained the most common TEAEs between 8 weeks and 6 months of follow-up, albeit occurring in only 10.0% (9/90) of participants with IBS and in 6.9% (42/607) of participants without IBS (Table 3).
Table 2 Summary of TEAEs within 8 weeks and between 8 weeks and 6 months of follow-up of RBL administration (safety population)Table 3 TEAEs by system organ class and preferred term with an incidence of ≥ 5% within 8 weeks and between 8 weeks and 6 months of follow-up of RBL administrationa (safety population)Serious TEAEs through 8 weeks after RBL administration were reported by 1 participant (1.1%) with IBS (pneumonia not considered related to RBL) and 26 participants (4.3%) without IBS (Table 2). In participants without IBS, most serious TEAEs were related to a preexisting condition (3.1%); 1 participant experienced a serious TEAE (ulcerative colitis flare) assessed by the investigator as possibly related to RBL. Between 8 weeks and 6 months of follow-up, serious TEAEs were reported by 3.3% (3/90) of participants with IBS and 3.6% (22/607) of participants without IBS. None of the events were considered related to RBL or its administration. Throughout the 6-month follow-up period, there were no TEAEs that led to study withdrawal or death in participants with IBS. Four deaths occurred in those without IBS (cardiac arrest (n = 1), cardiac failure (n = 1), spina bifida (n = 1), and pulmonary sepsis (n = 1), and 5 participants withdrew from the study. Based on a formal safety review by a medical monitor, Data Safety Monitoring Board, and the FDA, no serious TEAEs or deaths were adjudicated as being related to RBL or its administration.
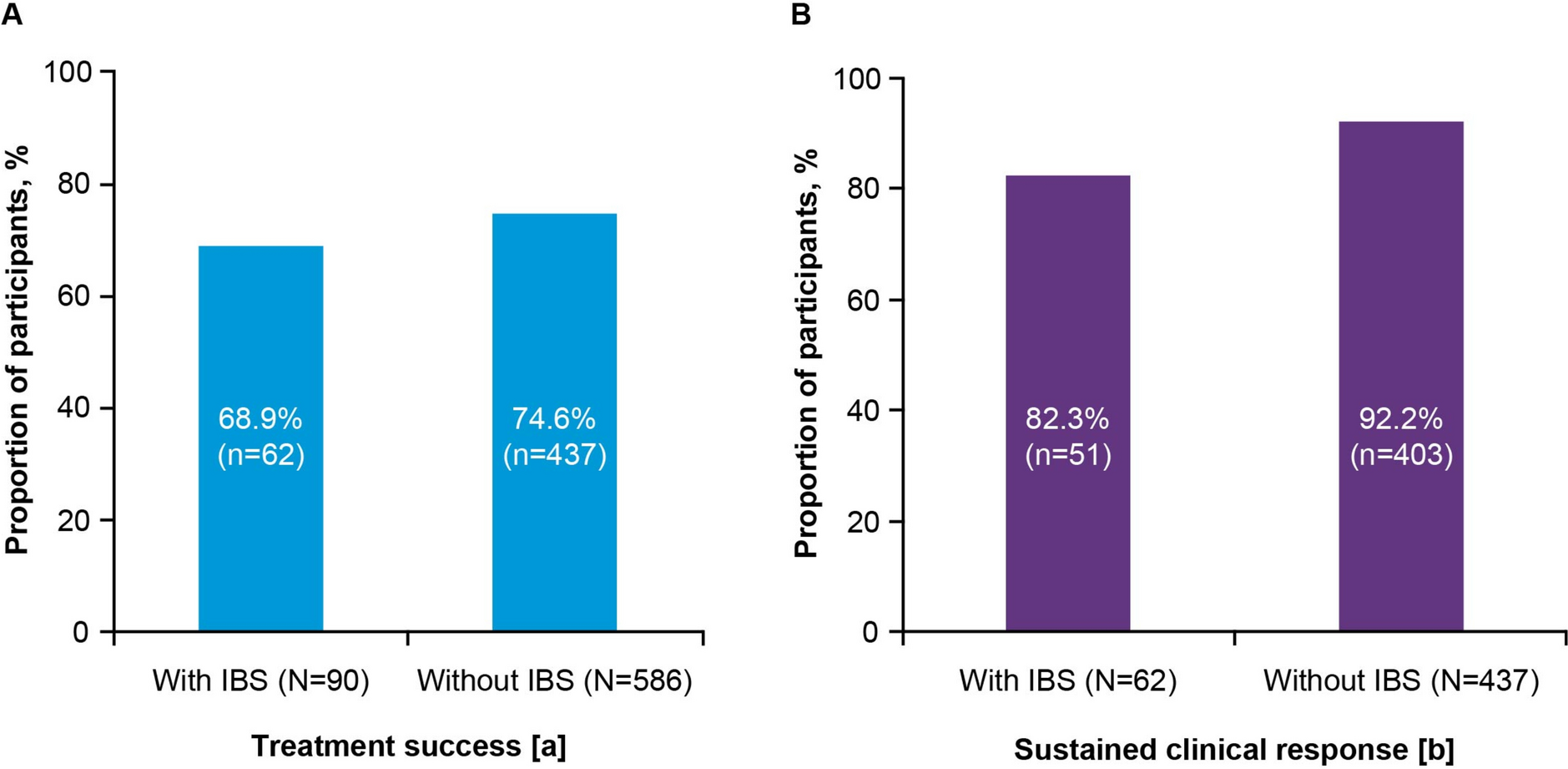
EfficacyIn the mITT population (n = 676), treatment success was achieved in 68.9% (62/90) of participants with IBS and 74.6% (437/586) of participants without IBS (Fig. 1a). Of the participants with treatment success, sustained clinical response through 6 months was maintained in 82.3% (51/62) and 92.2% (403/437) of participants with and without IBS, respectively (Fig. 1b).
Fig. 1
Efficacy outcomes within 8 weeks and between 8 weeks and 6 months of RBL administration (mITT population). a Treatment successa within 8 weeks of RBL administration. At 8 weeks, 24 participants (26.7%) with IBS experienced treatment failure (CDI recurrence) and 4 participants (4.4%) had indeterminatec outcomes. Among participants without IBS, 127 participants (21.7%) experienced treatment failure and 22 participants (3.8%) had indeterminate outcomes. b Sustained clinical responseb at 6 months in 8-week treatment responders. Five participants (8.1%) with IBS did not achieve a sustained clinical response and 6 participants (9.7%) had an indeterminate outcome. In the without IBS subgroup, 22 participants (5.0%) did not achieve a sustained clinical response, and 12 participants (2.7%) had an indeterminate outcome; CDI Clostridioides difficile infection, IBS irritable bowel syndrome, mITT modified intent-to-treat, RBL fecal microbiota, live-jslm.a Treatment success was defined as the absence of CDI diarrhea through 8 weeks after RBL administration. bSustained clinical response was defined as treatment success of the presenting rCDI and no new episodes of CDI through 6 months after treatment completion. cThe protocol-specified definition of treatment success or treatment failure was not met
Second Course of RBLOf the 24 participants with IBS and 127 participants without IBS who met the definition of treatment failure, 22 (91.7%) and 99 (78.0%) elected to receive a second course of single-dose RBL within 21 days of treatment failure.
Within 8 weeks of second course administration, 45.5% of participants with IBS and 37.4% of participants without IBS experienced TEAEs (Supplementary Table 3). Between 8 weeks and 6 months of second course administration, 31.8% of participants with IBS and 12.1% of participants without IBS experienced TEAEs. All TEAEs were mild or moderate in severity. Through 6 months after second course administration, no serious TEAEs were considered related to RBL or its administration in either subgroup. There were no study withdrawals or deaths in either subgroup. TEAEs following second course administration were similar to those following the first course (Supplementary Table 4).
Treatment success was achieved by 63.6% (14/22) of participants with IBS and 53.5% (53/99) of participants without IBS after receiving a second course of single-dose RBL (Supplementary Table 5). Among those who achieved treatment success after second course administration, 92.9% (13/14) of participants with IBS and 86.8% (46/53) of participants without IBS had a sustained response at 6 months.
Comments (0)