
Remember me


This population-level analysis was conducted using two models (dynamic and static), with assumptions aligned in order to estimate the cost-effectiveness of alternative treatment strategies with different shares of baloxavir and oseltamivir, taking into account the impact of antivirals on influenza transmission. A dynamic transmission model estimated the influenza incidence, i.e., proportion of the population in Japan who developed influenza. The outputs from the dynamic model were then used as input parameters for a static population-level decision tree model, which assessed the costs and benefits associated with each of the treatment strategies. This study was performed in line with the Japanese Guideline for Cost-Effectiveness Evaluation [14]. The base case analysis was conducted using a public healthcare payer’s perspective and a willingness-to-pay threshold (WTP) of JPY (Japanese yen) 5 million per quality-adjusted life year (QALY) gained [15].
An expert advisory panel was held in July 2024 with three experts (Dr. Takahiro Takazono, Dr. Naoki Hosogaya, and Dr. Ataru Igarashi), to validate clinical data sources and assumptions used in the model, covering the following topics: comparators, analysis design, model structure, incorporation of transmission model findings, influenza-related complications (probability of complications, hospitalization rate, and death), generic oseltamivir market share, scenario analyses, as well as modelling assumptions required to align methodological approaches used in the dynamic transmission model and the static cost-effectiveness model.
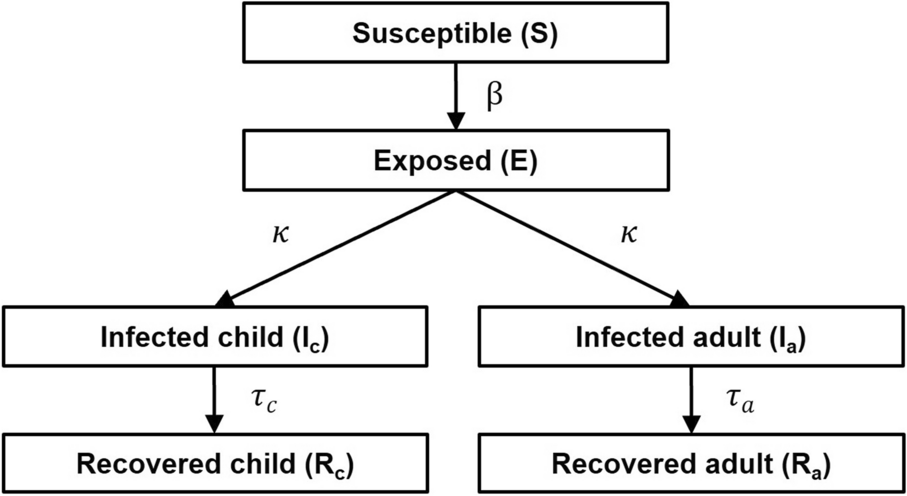
Susceptible, Exposed, Infected, Recovered (SEIR) Model OverviewA dynamic transmission SEIR model was developed for the presented analysis. This model predicts influenza incidence depending on the user-defined market shares of baloxavir and oseltamivir, as well as a proportion of patients without antiviral treatment. The model considers that treatment with each of the antivirals is associated with a certain duration of virus shedding, which has an impact on influenza transmission intensity in population. Duration of virus shedding in patients receiving baloxavir or oseltamivir and patients without antiviral treatment was informed by clinical trials [7, 9, 10]. Susceptible individuals started the model in compartment S. These individuals were then at risk of being exposed to influenza (moving to the compartment E), and subsequent development of influenza symptoms and becoming infectious (moving to the compartment I). After recovery from infection (moving to the compartment R), individuals were assumed to acquire full protection from an acquisition of a new infection until the end of the model simulation. Separate I and R compartments were considered for children (< 12 years old) and adults (≥ 12 years old), to reflect differences in the proportion of HR individuals, treatment strategies, and duration of virus shedding between these age groups. The SEIR model simulated influenza transmission in the population during the 2018/2019 influenza season. The season before the COVID-19 pandemic was selected to provide unbiased estimates, considering that post-pandemic influenza incidence is expected to be comparable to pre-pandemic levels, based on expert opinion and epidemiological evidence [16, 17]. The median incidence derived from 10,000 simulations of the SEIR model was used as a final incidence estimate and applied as an input for the cost-effectiveness model. The SEIR model structure is presented in Fig. 1. A description of the model equations, parameters, and a list of inputs are provided in Supplementary material Tables S1–S3. The SEIR model was programmed in Python, version 3.7.7.
Fig. 1
Dynamic transmission SEIR model structure. SEIR susceptible, exposed, infected, recovered, β influenza transmissibility, κ infection rate, τ recovery rate, c children, a adults. Recovery rate was also subgroup specific according to age, risk status, treatment, and presence of resistance
Cost-Effectiveness Model OverviewA previously published decision tree model [11, 12] was adapted to allow for the population-level analysis and incorporation of the infection rate simulated by the SEIR model. The starting model population reflected the total population in Japan. Branches representing the proportion of infected and non-infected individuals determined the subsequent costs and outcomes in the model. Infected patients were treated either with baloxavir or oseltamivir on the basis of the predetermined treatment strategies. Subsequent branches represented the clinical outcomes in patients with influenza, including recovery without complications, recovery with complications, and death. Patients were at risk of influenza-related complications, including pneumonia, bronchitis, sinusitis, and otitis media, as well as hospitalization due to complications, which had an impact on mortality, costs, and quality of life. Treated patients were also at risk of drug-related adverse events (AEs), and treatment failure due to resistance of the virus to the applied treatment. The model simulated influenza cases over the course of one influenza season, and accounted for the life years and QALYs lost due to influenza-related death over the lifetime horizon. Health and economic outcomes from the model were used to derive the incremental cost-effectiveness ratio (ICER) and the net monetary benefit (NMB) for the evaluated comparison of strategies. The ICER was calculated as the ratio of incremental costs to incremental QALYs, where both values had the same sign. For cases where the intervention was both more effective and less costly (dominant), or less effective and more costly (dominated), the ICER was not reported. The NMB was calculated by multiplying the incremental QALYs by the WTP threshold and subtracting the incremental costs (or adding cost savings). The cost-effectiveness model was programmed using Microsoft Excel 365.
The cost-effectiveness model structure is presented in Fig. 2. A description of model parameters is provided in subsections below, and input values are provided in Supplementary material Tables S4–S7.
Fig. 2
Cost-effectiveness model structure. AE adverse event
Treatment StrategiesThe modelled treatment strategies were defined on the basis of the estimated market shares of baloxavir and oseltamivir, which are the oral anti-influenza treatments used in Japan [18]. For children (< 12 years old), both strategies considered 20% baloxavir and 80% oseltamivir based on current clinical practice. For patients ≥ 12 years old, the alternative treatment strategies included (1) 40% baloxavir and 60% oseltamivir, and (2) 50% baloxavir and 50% oseltamivir. Other NAIs (zanamivir, peramivir, and laninamivir) were not considered in this analysis as a result of the lack of data on duration of virus shedding.
Population CharacteristicsThis analysis considered the full Japanese population and the following subpopulations: children (< 12 years old), adolescents and adults (between 12 and 64 years old), and elderly (≥ 65 years old).
Subpopulations were categorized into subgroups according to the presence of known risk factors for influenza complications (defined as OwH or HR). Risk factors included one or more of the following: blood disorders, chronic lung diseases, compromised immune system, endocrine disorders, morbid obesity, heart diseases, metabolic disorders, and neurological or neurodevelopmental disorders. HR patients also included women who were 2 weeks post-partum, children aged < 6 years old, and long-term care facilities residents, in line with the previous clinical studies for baloxavir and the established risk factors for influenza complications [19,20,21].
Studies by Shibata et al., Yamada et al., Deguchi et al., JammNet database, and MHLW [22,23,24,25,26] informed the proportion of the HR population in adults and elderly, in line with the previous analysis in HR population [11]. For children, it was assumed that only individuals aged 0–5 years old are at high risk of complications, and all individuals aged 6–11 were considered as OwH. The corresponding prevalence of HR conditions was applied to the Japanese demographic data for 2023 [27]. It was estimated that the total study population included 5% of OwH children, 4% of HR children, 50% of OwH adults, 12% of HR adults, 15% of OwH elderly, and 14% of HR elderly.
Influenza Incidence EstimationThe proportion of patients infected with influenza under the alternative treatment strategies was informed by the SEIR model, and was consistent with real-world evidence [28] and expert opinion. There were 11.7 million people infected with influenza in the 2018/2019 influenza season in Japan (9% of the total population) [28]. This is consistent with the incidence predicted by the model (10%) when the baloxavir share in patients ≥ 12 years is set to 50%, which corresponds to the estimated market share for baloxavir in the 2018/2019 season [18]. In the hypothetical alternative scenario with 40% baloxavir share in patients ≥ 12 years, influenza incidence was estimated in SEIR at 12%. Then, predicted incidence rates for each strategy were used to calculate incidence rate in children (< 12 years old) and adults (≥ 12 years old), considering the observed age distribution of influenza cases for the 2018/2019 season [28, 29]. The obtained incidence rates for children and adults were applied to the 2023 population estimates in Japan [27], in order to capture the current demographic structure of population, while maintaining the age distribution of influenza cases as reported for the target 2018/2019 influenza season.
Clinical DataResistance rates to baloxavir and oseltamivir were informed by the 2018/2019 season report of the National Institute of Infectious Diseases (NIID), currently the Japan Institute of Health and Sciences (JIHS) [28], including only loss of viral susceptibility observed in patients without treatment by each corresponding antiviral (i.e., including only pre-treatment resistance). As it was assumed that emergence of resistant strains in patients undergoing treatment was explicitly captured in the clinical trial results, they were not considered in the estimation of resistance rates used as the model inputs.
Probabilities of influenza-related complications and drug-related AE rates were derived from pivotal clinical trials (miniSTONE-2, NCT03629184 for children, CAPSTONE-1, NCT02954354 for OwH adults, CAPSTONE-2, NCT02949011 for HR adults and elderly) [7, 9, 30]. Additionally, in order to incorporate the most comprehensive evidence available to date, the previous network meta-analysis (NMA) for an adult HR population was applied to derive the probability of bronchitis for oseltamivir and no antiviral [31].
The probability of hospitalization due to complications in OwH and HR adults and elderly was informed by the JammNet database analysis [11, 12]. For OwH and HR children, an increased risk of hospitalization was applied, with probabilities estimated for corresponding subgroups of adults scaled up by a risk ratio of 2.99, derived from Yokomichi et al. [32].
Two types of mortality were included in the model: background mortality, and influenza-related mortality due to complications (regardless of the hospitalization status). Background mortality was based on the general Japanese population life tables stratified by age and sex [27]. Additionally, for the HR population, the probability of death was adjusted to account for the presence of HR conditions using data from the 2017 Demographic Survey [33]. Influenza-related mortality due to complications was assumed to occur only in patients experiencing pneumonia or bronchitis, regardless of treatment status. For adults and the elderly, the probability of influenza-related death was estimated using a study by Miyashita et al. [34]. Then the obtained estimates were adjusted to take into account the higher risk of death in HR patients, using the risk ratio for HR patients vs OwH patients reported by Hoshi et al. [35]. The probability of influenza-related death in HR children was estimated using the risk ratio for HR children vs HR adults, based on the data reported by Burch et al. [36]. Finally, the probability of influenza-related death in OwH children was set to 0%, which was considered acceptable by the expert panel, given the lack of data and very low mortality observed in this subgroup in clinical practice.
Cost DataIn line with the Japanese guidelines for cost-effectiveness studies [14], costs were estimated from the healthcare payer perspective for the base case. Influenza management costs, including physician visits and prescription fees, were sourced from the Ministry of Health, Labour and Welfare (MHLW) Medical fee index for 2024 [37].
Drug acquisition costs for baloxavir and oseltamivir (including capsule and dry syrup forms, branded and generic) were extracted from the MHLW drug price list [38]. Dosages were aligned with treatment labels [20, 39, 40], and adjusted for patients’ age and weight distribution. Distribution of influenza cases among age groups was based on 2018/2019 season data reported by the NIID, Japan [28]. Weight distribution for children was sourced from The National Health and Nutrition Survey in Japan, 2019 [41]. Weight distribution for adults was also applied, to adjust baloxavir dosage for patients with a weight of ≥ 80 kg, in line with the dosing criteria used in clinical trials and the approved product label [7, 9, 20]. The proportion of patients with a weight of ≥ 80 kg was considered the same for all adults and elderly patients, and estimated using the phase 3 clinical trials data [9] and stratification of study population. Both branded and generic oseltamivir were considered for the cost estimation. For capsules, the share of branded and generic oseltamivir was 50%/50%, respectively, for the dry syrup form, these were 60%/40%, respectively [18].
Costs associated with AEs, complications, and hospitalizations in adults and elderly were sourced from the previous JammNet database analysis [11, 12], and adjusted to 2024 price levels using the revision rates reported by MHLW [42,43,44,45]. Costs for OwH and HR children were calculated on the basis of a percentage change (− 53%) between children and adult’s hospitalization cost, derived from Sruamsiri et al. [46]. A scenario considering a societal perspective was explored, taking into account the costs of lost productivity. Productivity loss inputs were informed by data on influenza-related work absenteeism from the CAPSTONE-2 trial [9], average wage estimated using the MHLW data [47, 48], as well as employment rates and number of monthly working hours sourced from the Labour Force Survey in Japan [49].
Quality-of-Life DataBaseline quality-of-life data were derived from studies by Shiroiwa et al. who reported the Japanese population norms, based on EQ-5D-5L [50, 51]. Further, utility decrements were applied, taking into account the presence of HR conditions, influenza symptoms, influenza-related complications, and drug-related AEs.
Adults and elderly in the HR subgroups were assumed to have a lower quality of life compared with OwH individuals of the same age group, in line with the previous analysis in HR population [11]. Disutilities due to HR conditions were informed by the relevant literature [52,53,54,55,56]. No disutility due to risk conditions was applied for HR children, as this subgroup was defined according to age, and assumed to include only the general population aged 0–5 years old.
All patients with influenza symptoms experienced loss of quality of life until alleviation of symptoms. Disutility due to influenza symptoms for adults and elderly was informed by CAPSTONE-1 and CAPSTONE-2 clinical trials [7, 9], in line with previous studies for OwH and HR populations, respectively [11, 12]. As a result of the lack of data for children, it was assumed that the utility decrement in OwH and HR children is the same as in OwH and HR adults, respectively. Duration of symptoms in patients treated with baloxavir was sourced from the miniSTONE, CAPSTONE-1, and CAPSTONE-2 clinical trials [7, 9, 30]. Duration of symptoms in patients treated with oseltamivir and those without treatment was estimated using the data from the previous NMAs [31, 57].
Duration of influenza complications and associated utility decrements were sourced from a study by Burch et al. [36]. Given lack of data, the duration of otitis media was assumed to be equal to the duration of bronchitis, and patients with sinusitis were assumed to have the same utility decrement as patients with respiratory tract infections.
The duration of drug-related AEs for baloxavir and oseltamivir was informed by the open-label study for children [58], as well as CAPSTONE-1 and CAPSTONE-2 clinical trials, for adults and elderly [7, 9]. The utility decrement for AEs was informed by a study by Tappenden et al. [59].
Quantifying UncertaintyDeterministic sensitivity analysis (DSA) was conducted to identify the parameters with the largest impact on the cost-effectiveness model results. The combined uncertainty from all parameters in the model was characterized using probabilistic sensitivity analysis (PSA), with results represented using a scatter plot on the cost-effectiveness plane. DSA and PSA were performed only for the cost-effectiveness model input parameters associated with uncertainty, with ranges of variation informed by the literature data when available or based on an assumed percentage variation (e.g., ± 10% or ± 25%). The values applied in the DSA and PSA are presented in Supplementary material Table S4-S7, alongside the base case values.
Model assumptions, which are likely to have an impact on the analysis results, and which could not be included in the DSA or PSA, were tested using scenario analyses, for population-level outcomes. The choice of scenario analysis was discussed and agreed with clinical experts in Japan. Scenario 1 explored the impact of excluding the effect of treatment on disease transmission by setting the equal incidence of influenza in both of the modelled treatment strategies. As a conservative assumption, the lower incidence (predicted for a strategy with 50% of baloxavir in patients ≥ 12 years) was applied for both strategies in this scenario. Additionally, scenarios 2 and 3 were performed to explore the impact of the further increase in the share of baloxavir use for treatment of adults and elderly, up to 60% to 70%. Scenario 4 considering a societal perspective was also explored, in order to include benefits of antiviral treatments for productivity, which was in line with the Japanese Guideline for Cost-Effectiveness Evaluation [14].
Ethical ApprovalThis article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Comments (0)