
Remember me

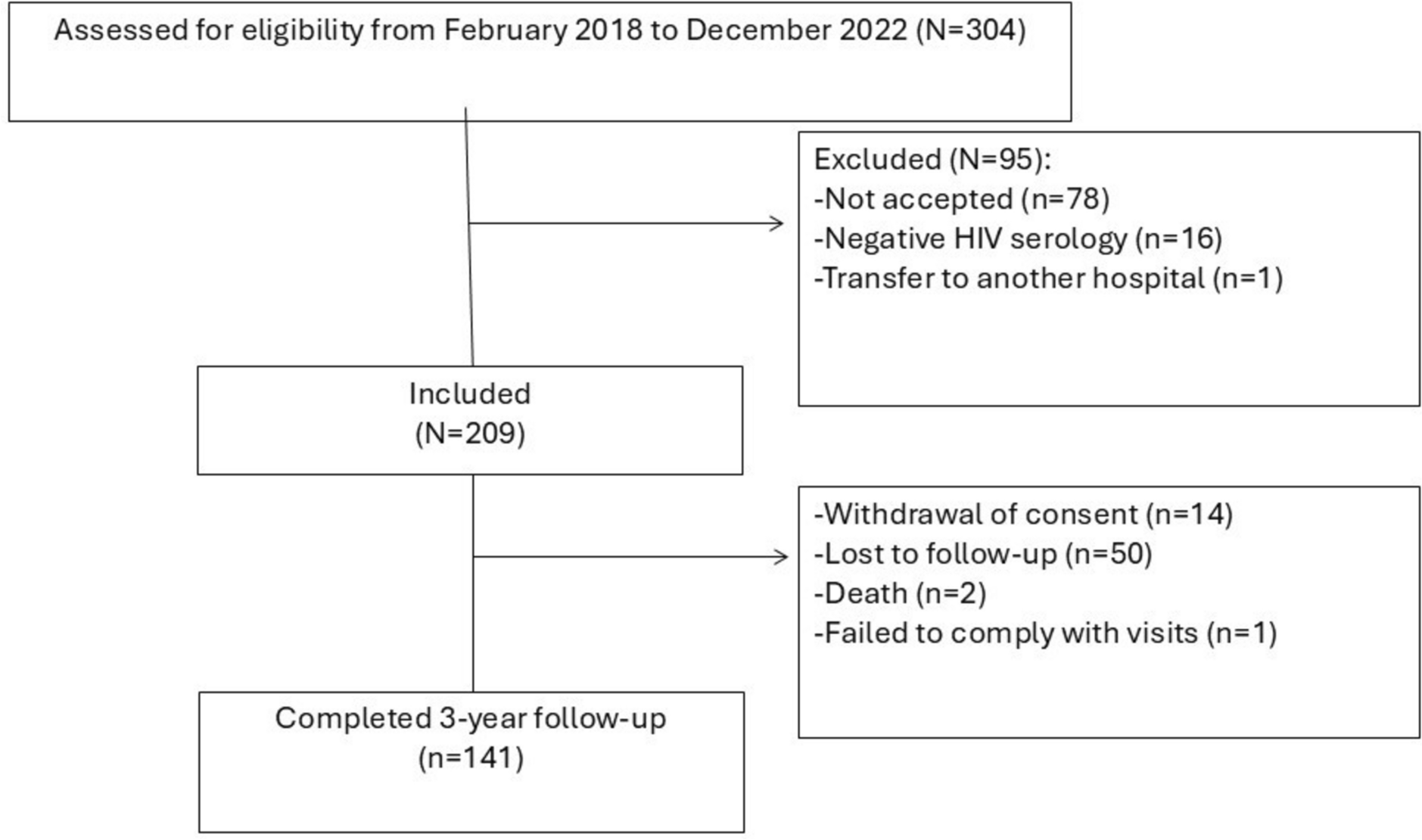
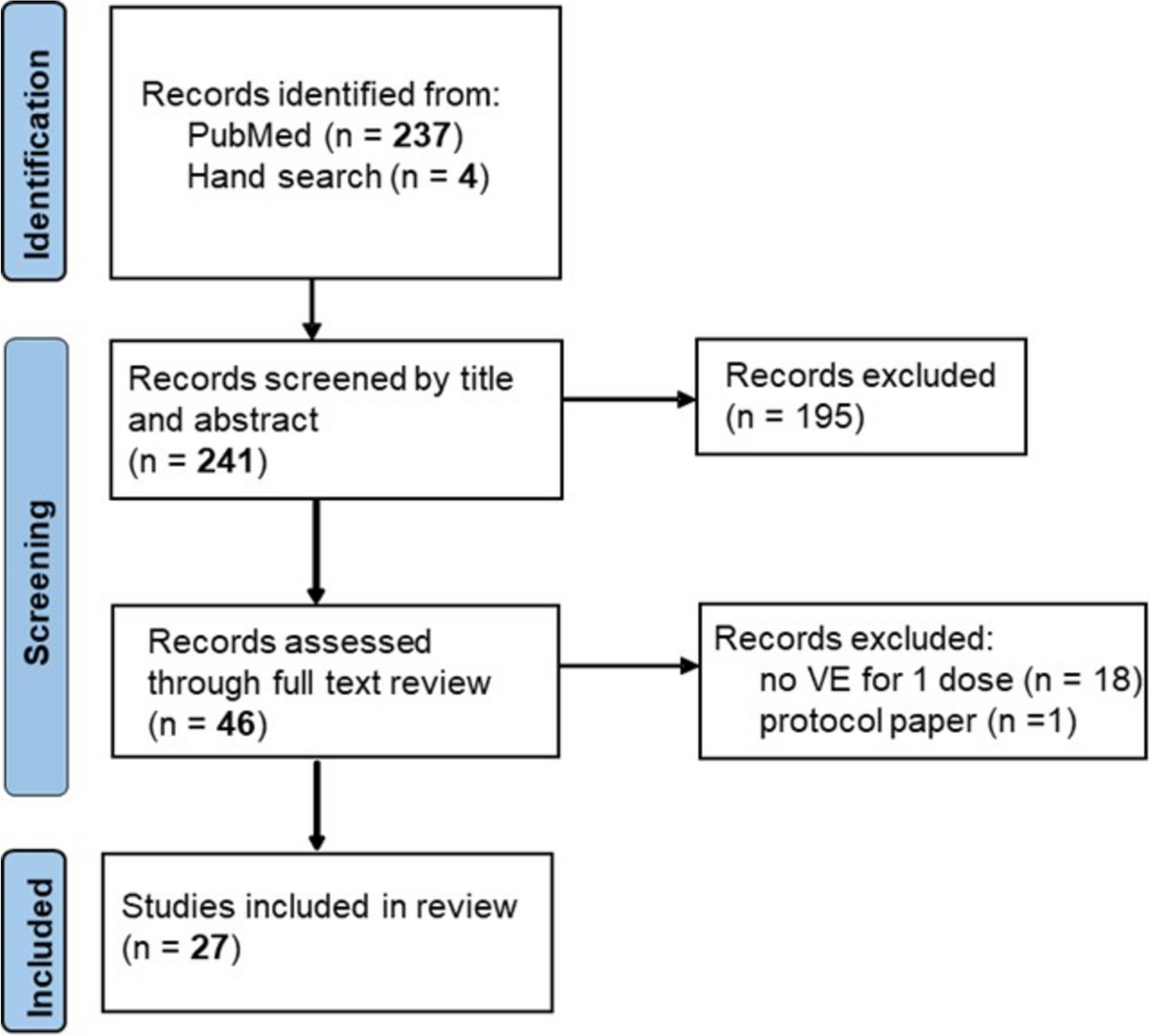

The database search identified a total of 19,991 publications. Following de-duplication, 13,611 abstracts were screened, and 470 records were retained for full-text review. Overall, 49 publications (30 journal articles and 19 conference abstracts) reporting 41 unique studies [15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53] were included. Most included studies (30) were published after 2017, the year of publication of the prior SLR by Waziry et al. [5] The PRISMA flow diagram is presented in Fig. 1.
Fig. 1 Summary of Included Studies
Summary of Included StudiesCharacteristics of the included studies are presented in Table 2 (a complete summary table is provided in the Supplementary Material, Table S8). There were 10,563 enrolled participants among the 41 included studies, ranging from 28 [45] to 2173 [25] participants per study (median 133, mean 258). All 41 included studies were cohort studies; 31 were retrospective, eight were prospective, and two studies were a mixture of retrospective and prospective design elements.
Table 2 Study characteristicsPatient demographics and clinical characteristics were comparable within the main inclusion and exclusion criteria. Most studies (24) were conducted in Asia (Japan, South Korea, and Taiwan); nine were conducted in Europe (France, Italy, Poland, Romania, and Spain); one each in the USA, Canada, and Egypt; one in Europe and the USA; and four did not report the country. The median age of study participants for all studies was above 55 years (range 56–74 years). Sex ranged from 39.3% [20] to 87% [48] male; only one conference abstract reported demographic characteristics [40]. No studies reported on race, ethnicity, or rheumatoid arthritis (a predefined comorbidity of interest) at baseline.
The eligible treatment sequence for all patients was curative HCC treatment followed by DAA or comparison treatment for HCV. The most frequently reported types of prior HCC treatment were surgery/resection (20 studies, median 34.6%, range 3.2–100%), ablation (20 studies, median 67%, range 13–100%), and radiation therapy (3 studies, median 6.1%, range 2–18%); patients with prior liver transplantation were not eligible for this review because HCV-infected patients with liver transplantation represent a different patient population than those without liver transplantation.
The intervention for all included studies was IFN-free DAA (second-generation DAAs). In four studies, some patients in the IFN group also may have received one of three IFN-containing DAA regimens (telaprevir, simeprevir, or vaniprevir) (Kinoshita 2019 [25], Mashiba 2018 [29], Nagata 2017 [36], and Tahata 2020 [43]). Thirty-four studies compared DAAs with a single comparator group and seven studies compared DAAs with two comparator groups (DAA versus IFN versus no antiviral treatment). Study-specific details for treatment characteristics are provided in the Supplementary Material (Table S9).
Studies Comparing DAA Versus IFNSeventeen studies compared IFN-free DAA regimens with IFN (6802 participants), including seven three-group studies that also evaluated no antiviral therapy (Table 2). Most studies were conducted in Asia (Japan, n = 8; Taiwan, n = 3; and South Korea, n = 1); one each in the USA and Europe (Italy); and three did not report the country. The median age ranged from 60.2 [26] to 74.1 [24, 25] years. One study included 9% of patients who had HBV coinfection (Chi 2019 [20]). No study reported including patients with HIV coinfection at baseline. Total study duration ranged from 38 [20] to 298 [35] months for 12 studies; five studies did not report a total study duration.
The DAA treatment groups included any combination or mixture of the 12 eligible DAAs (Table 1), with or without ribavirin (RBV). The length of DAA treatment, when reported, was 12 or 24 weeks. The IFN group comprised treatment with IFN or Peg-IFN, with or without RBV. The length of IFN treatment, when reported, was 12 to 48 weeks. In four studies, some patients in the IFN group also may have received one of three IFN-containing DAA regimens (telaprevir, simeprevir, or vaniprevir) (Kinoshita 2019 [25], Mashiba 2018 [29], Nagata 2017 [36], and Tahata 2020 [43]).
Studies Comparing DAA Versus No DAAFourteen studies (1766 participants) compared IFN-free DAA regimens with a no DAA comparator group; all were two-group studies (Table 2). Seven studies were conducted in Asia (Japan, n = 6; Taiwan, n = 1); five in Europe (France, n = 2; and one each in Italy, Poland, and Romania); one in Africa (Egypt); and one in Europe and the USA. The median age ranged from 56.7 [21] to 77 [27] years. No patient was reported to have HIV coinfection; one study included 3 (2%) with HBV coinfection [27]. Total study duration was reported by only five studies, ranging from 18 [34] to 191 [32] months, with nine studies not reporting a total study duration.
The DAA treatment groups included any combination or mixture of the 12 eligible DAAs (Table 1), with or without ribavirin (RBV). The length of DAA treatment, when reported, was 12 or 24 weeks. For all studies, the no DAA group was reported only as not receiving DAAs with no indication whether IFN or another antiviral treatment was administered.
Studies Comparing DAA Versus No Antiviral TherapySeventeen studies (4452 participants) compared IFN-free DAA regimens with no antiviral therapy, including seven three-group studies that also evaluated IFN therapy (Table 2). Most studies were conducted in Asia (Japan, n = 6; Taiwan, n = 3; and South Korea, n = 1); four in Europe (one each in France, Italy, Romania, and Spain); one in Canada; and two did not report the country. The median age ranged from 61.0 [47] to 74.1 [24] years. One study included < 10% of patients who had HIV coinfection (Perello 2019 [40]). Total study duration ranged from 18 [40] to 209 [31] months, with eight studies not reporting a total study duration.
The DAA treatment groups included any combination or mixture of the 12 eligible DAAs (Table 1), with or without ribavirin (RBV), for 12 or 24 weeks. For all studies, the comparison group was described as receiving no antiviral therapy or no treatment.
Summary of Reported Outcome DataMost studies reported the risk of HCC recurrence assessed by imaging with computed tomography (CT) or magnetic resonance imaging (MRI), or ultrasonography (US). Study-specific HCC recurrence outcome definitions are provided in the Supplementary Material (Table S10). Outcomes were analyzed by comparison group: IFN, no DAA (as reported by study authors as not receiving DAAs with no indication whether IFN or another antiviral therapy was administered, or no antiviral therapy was administered), and no antiviral therapy (explicitly reported by study authors as not receiving any antiviral therapy). Most studies reported the risk of HCC recurrence as a proportion at 12 months, 24 months, or longest follow-up; 13 of 17 studies comparing DAA versus IFN, 14 of 14 studies comparing DAA versus no DAA, and 15 of 17 studies comparing DAA versus no antiviral therapy (Supplementary Material Table S11). Only two studies reported HCC recurrence at 18 months (Muzica 2022 [34] and Perello 2019 [40]), each of which evaluated a different comparator and neither was eligible for the primary analysis, thus precluding meta-analysis for this timepoint. Of 37 studies that reported the risk of HCC recurrence as a proportion, 23 studies were eligible for primary analysis and 14 studies were included in sensitivity analysis only.
One study comparing DAA versus IFN, five studies comparing DAA versus no DAA, and four studies comparing DAA versus no antiviral therapy reported incidence of HCC recurrence (Table 3). Two studies comparing DAA versus IFN, five studies comparing DAA versus no DAA, and four studies comparing DAA versus no antiviral therapy reported HCC recurrence as a hazard ratio (Table 4). The follow-up times for outcomes reported as incidence or hazard ratios for HCC recurrence differed across studies precluding meta-analysis.
Table 3 Studies reporting the incidence of HCC recurrenceTable 4 Studies reporting the hazard ratio for HCC recurrence between treatment groupsRisk of HCC Recurrence: Meta-Analysis ResultsStudies Comparing DAA Versus IFNAt 12 months follow-up
Five studies (765 patients) reported risk of HCC recurrence at 12 months, which ranged from 0 to 57 recurrences per study for patients treated with IFN-free DAA regimens (AR 28 per 100 individuals) and 0 to 61 recurrences per study for patients treated with IFN (AR 23 per 100 individuals). The combined RR for HCC recurrence was 1.29 [95% CI 0.69, 2.40] (Fig. 2), indicating no difference between DAA and IFN with considerable statistical heterogeneity (I2 statistic 66.6%) and imprecision (i.e., wide confidence interval).
Fig. 2
Random effects model results for HCC recurrence at 12 months: primary analysis. Forest plot for risk ratio of HCC recurrence, DAA versus comparators at 12 months. Risk ratio < 1 favors DAA therapy, risk ratio > 1 favors comparator. Confidence intervals not including 1 indicate significant difference between groups. Studies with DAA versus two comparator groups are indicated as a interferon treatment group and b no antiviral therapy treatment group. CI confidence interval, DAA direct-acting antiviral, HCC hepatocellular carcinoma
Analysis using the fixed effect model was similar to the primary analysis using the random effects model. The fixed effect combined RR for HCC recurrence was 1.22 [95% CI 0.97, 1.54] (Supplementary Material, Fig. S1), indicating no increased risk between DAA and IFN with considerable statistical heterogeneity (I2 statistic 70.5%). No sensitivity analysis was conducted for this outcome because all studies at this timepoint were included in the primary analysis.
At 24 months follow-up
Four studies (633 patients) reported risk of HCC recurrence at 24 months. HCC recurrence ranged from 1 to 88 recurrences per study for patients treated with DAA (AR 43 per 100 individuals) and 2 to 95 recurrences per study for patients treated with IFN (AR 53 per 100 individuals). The combined RR for HCC recurrence was 0.88 [95% CI 0.56, 1.39] (Fig. 3), indicating no difference between DAA and IFN with substantial statistical heterogeneity (I2 statistic 77.8%).
Fig. 3
Random effects model results for HCC recurrence at 24 months: primary analysis. Forest plot for risk ratio of HCC recurrence, DAA versus comparators at 24 months. Risk ratio < 1 favors DAA therapy, risk ratio > 1 favors comparator. Confidence intervals not including 1 indicate significant difference between groups. Studies with DAA versus two comparator groups are indicated as a interferon treatment group and b no antiviral therapy treatment group. CI confidence interval, DAA direct-acting antiviral, HCC hepatocellular carcinoma
Analysis using the fixed effect model was similar to the primary analysis using the random effects model. The fixed effect combined RR for HCC recurrence was 1.02 [95% CI 0.88, 1.18] (Supplementary Material, Fig. S2), indicating no increased risk between DAA and IFN with substantial statistical heterogeneity (I2 statistic 69.9%). The inclusion of one additional study that was not eligible for primary analysis, Yoshida 2017 [53] (DAA exposure not described), did not impact the meta-analysis results (random effects RR 0.85 [95% CI 0.57, 1.25], Supplementary Material, Fig. S3; fixed effect RR 1.00 [95% CI 0.86, 1.15], Supplementary Material, Fig. S4).
At longest follow-up
Nine studies (1557 patients) reported risk of HCC recurrence, which ranged from 1 to 108 recurrences per study for patients treated with DAA (AR 37 per 100 individuals) and 3 to 136 recurrences per study for patients treated with IFN (AR 59 per 100 individuals). The combined RR for HCC recurrence was 0.67 [95% CI 0.51, 0.88] (Fig. 4), indicating favorable results for DAA therapy compared with IFN with considerable statistical heterogeneity (I2 statistic 78.7%).
Fig. 4
Random effects model results for HCC recurrence at longest follow-up: primary analysis. Forest plot for risk ratio of HCC recurrence, DAA versus comparators at longest reported follow-up. Risk ratio < 1 favors DAA therapy, risk ratio > 1 favors comparator. Confidence intervals not including 1 indicate significant difference between groups. Studies with DAA versus two comparator groups are indicated as a interferon treatment group and b no antiviral therapy treatment group. CI confidence interval, DAA direct-acting antiviral, HCC hepatocellular carcinoma
Fixed effect model and sensitivity analyses also favored DAA therapy compared with IFN. The fixed effect combined RR for HCC recurrence was 0.70 [95% CI 0.63, 0.78] (Supplementary Material, Fig. S5), indicating no increased risk between DAA and IFN with substantial statistical heterogeneity (I2 statistic 78.7%). The inclusion of four additional studies that were not eligible for primary analysis, namely Mashiba 2018 [29] (< 12 months follow-up in DAA group), Woo 2019 [51] (< 12 months follow-up in DAA group and DAA exposure not described), Yasui 2017 [52] (< 12 months follow-up in DAA group and DAA exposure not described), and Yoshida 2017 [53] (DAA exposure not described) did not impact the meta-analysis results (random effects RR 0.65 [95% CI 0.52, 0.82], Supplementary Material, Fig. S6; fixed effect RR 0.63 [95% CI 0.57, 0.69], Supplementary Material, Fig. S7). Funnel plot examination did not suggest small study effects due to potential publication bias (Egger’s test p value = 0.197, Supplementary Material, Fig. S8).
Studies Comparing DAA Versus No DAAAt 12 months follow-up
Three studies (374 patients) compared IFN-free DAA regimens versus no DAA (as reported by study authors as not receiving DAAs with no indication whether IFN or another antiviral therapy was administered, or no antiviral therapy was administered) at 12 months (Fig. 2). Results from these studies reported the risk of HCC recurrence ranging from 2 to 20 recurrences per study for patients treated with DAA (AR 18 per 100 individuals) and 12 to 25 recurrences per study for patients receiving no DAAs (AR 27 per 100 individuals). The combined RR for HCC recurrence was 0.55 [95% CI 0.25, 1.23] (Fig. 2), indicating favorable results for DAA therapy compared with no DAA therapy with considerable statistical heterogeneity (I2 statistic 65.7%).
With the inclusion of two additional studies that were not eligible for primary analysis, Ikenaga 2022 [23] and Warzyszynska 2018 [50] (DAA exposure not described), the sensitivity analysis results significantly favored DAAs (random effects RR 0.59 [95% CI 0.37, 0.94], Supplementary Material, Fig. S9; fixed effect RR 0.68 [95% CI 0.49, 0.93], Supplementary Material, Fig. S10).
At 24 months follow-up
Six studies (727 patients) reported risk of HCC recurrence at 24 months. HCC recurrence ranged from 1 to 24 recurrences per study for patients treated with DAA (AR 20 per 100 individuals) and 5 to 46 recurrences per study for patients not treated with DAA (AR 38 per 100 individuals). The combined RR for HCC recurrence was 0.67 [95% CI 0.51, 0.86] (Fig. 3), indicating favorable results for DAA compared with no DAA with no statistical heterogeneity (I2 statistic 0.0%).
Results using the fixed effect model were the same as primary analysis results using the ran
Comments (0)