
Remember me





Juvenile polyposis syndrome (JPS) is an autosomal dominant condition with incomplete penetrance and an estimated worldwide incidence of 1 in 100,000. Up to 45% of individuals diagnosed with JPS have mutations in the SMAD4 or BMPR1A genes.1 The syndrome is diagnosed when 1 of 3 clinical criteria are met, ie, more than 5 juvenile polyps in the colon and rectum, juvenile polyps in other parts of the gastrointestinal tract, or any number of juvenile polyps and a positive family history.2
Given the high number of polyps, most patients are symptomatic by the age of 20 years. Rectal bleeding is the most common presenting symptom. Other symptoms include prolapse, abdominal pain, diarrhea, and anemia.3 Our patient had a previous diagnosis of ulcerative colitis (UC) and was subsequently found with JPS.
A patient with UC and a rare undiagnosed underlying condition such as JPS presents with diagnostic difficulty as there is significant overlap in associated symptoms. Moreover, both conditions are independently associated with increased risk of cancer. In UC, the duration and extent of inflammation have been associated with increased risk of colorectal cancer (CRC).4,5 Specifically, mucosal inflammation evidenced on histologic and endoscopic examination were associated with an increased risk of colorectal neoplasia.5
For individuals with JPS, the mean age of diagnosis of CRC is 44 years and the cumulative lifetime risk is 38.7%. In addition, JPS confers a lifetime risk of gastric and duodenal cancer of 11%–20%.6,7 Those with UC have a 2.4 fold increased risk of developing CRC.8 The cumulative incidence of CRC was 2.5% after 20 years and 7.6% after 30 years of disease.9 However, to date, there have been no studies to quantify the risk of CRC in patients with both JPS and UC.
CASE REPORTA 27-year-old man with a medical history of UC diagnosed in 2011. He discontinued medications due to insurance costs and then was admitted to the hospital for severe anemia, shortness of breath, fatigue, and maroon-colored stools up to 9 times a day. He was found to be tachycardic to 105 bpm and normotensive with a blood pressure of 120/67.
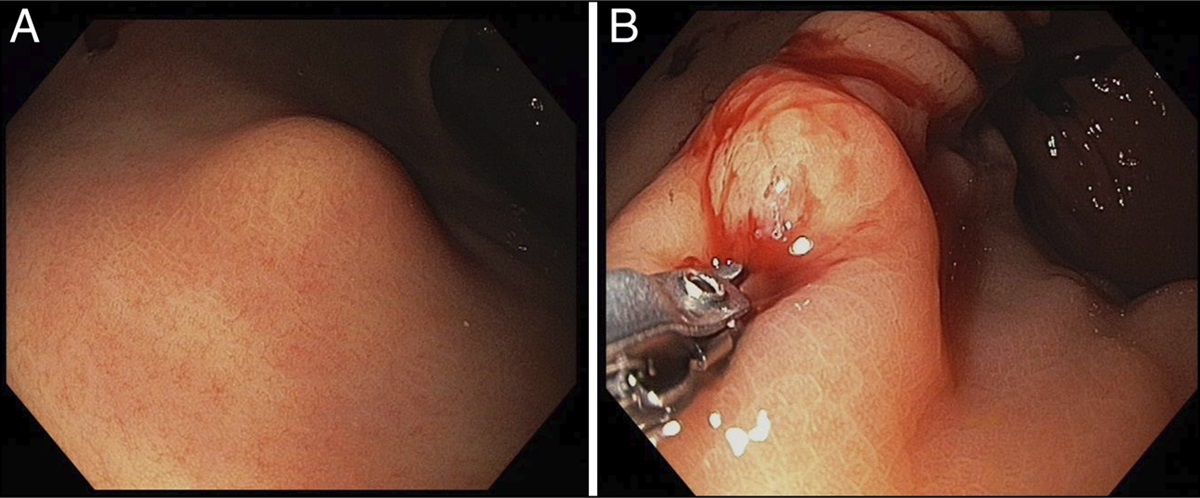
His hemoglobin was 5 g/dL, ferritin was 1 ng/mL, and iron was 14 μg/dL. Computed tomography (CT) angiography revealed mild bowel wall thickening of the rectosigmoid colon and concern for active extravasation. He received a total of 3 units packed red blood cells and intravenous iron supplementation. His fecal calprotectin was 367 μg/g. A carcinoembryonic antigen was within normal limits. Subsequent upper endoscopy revealed 3 gastric polyps which were resected. Colonoscopy revealed numerous hamartomatous polyps throughout the entire colon, the largest measuring 80 mm (Figure 1). Segmental mucosal biopsies were performed, and polypectomy was performed on several large representative polyps. Histologically, the stomach polyp was both hamartomatous and hyperplastic. The colon polyps were juvenile and inflammatory polyps with dysplasia ranging from indeterminate in the ascending colon, low grade in the descending colon, and high grade in the rectal biopsy with p53 null expression and loss of SMAD4 expression throughout. Mucosal biopsies from the left colon and rectum revealed hyperplastic change but no inflammation or colitis.
 Figure 1.:
Figure 1.: Colonoscopy showing multiple polyps in the (A) ascending, (B) descending, and (C) sigmoid colon. (D) Another view of single polyp in the sigmoid colon.
Following colonoscopy, the patient was deemed stable for discharge with a short interval CT scan recommended while awaiting biopsy results to assess for new inflammation as the patient continued to experience hematochezia.
In the initial 2011 colonoscopy, when he was first evaluated for UC, multiple polyps were seen throughout the gastrointestinal tract, including the cecum and sigmoid areas. Multiple biopsies resulted as inflamed hamartomatous polyps; however, no dysplasia was seen at that time. Repeat colonoscopy in 2013 and 2014 showed no evidence of inflammation or dysplasia near the terminal ileum; however, there were persistent inflamed hamartomatous polyps at the cecum and splenic flexure. In colonic mucosa, mucosal biopsies revealed crypt architectural distortion, advanced chronic active inflammation, and granulation without dysplasia. Prior esophagogastroduodenoscopy performed in 2011 did not reveal any polyps, only nonspecific gastritis and duodenitis. Patient was started on mesalamine afterward in 2016 which was stopped in 2019 due to lack of insurance coverage. Since 2016, in the interim, he has had multiple bowel movements daily but without hematochezia.
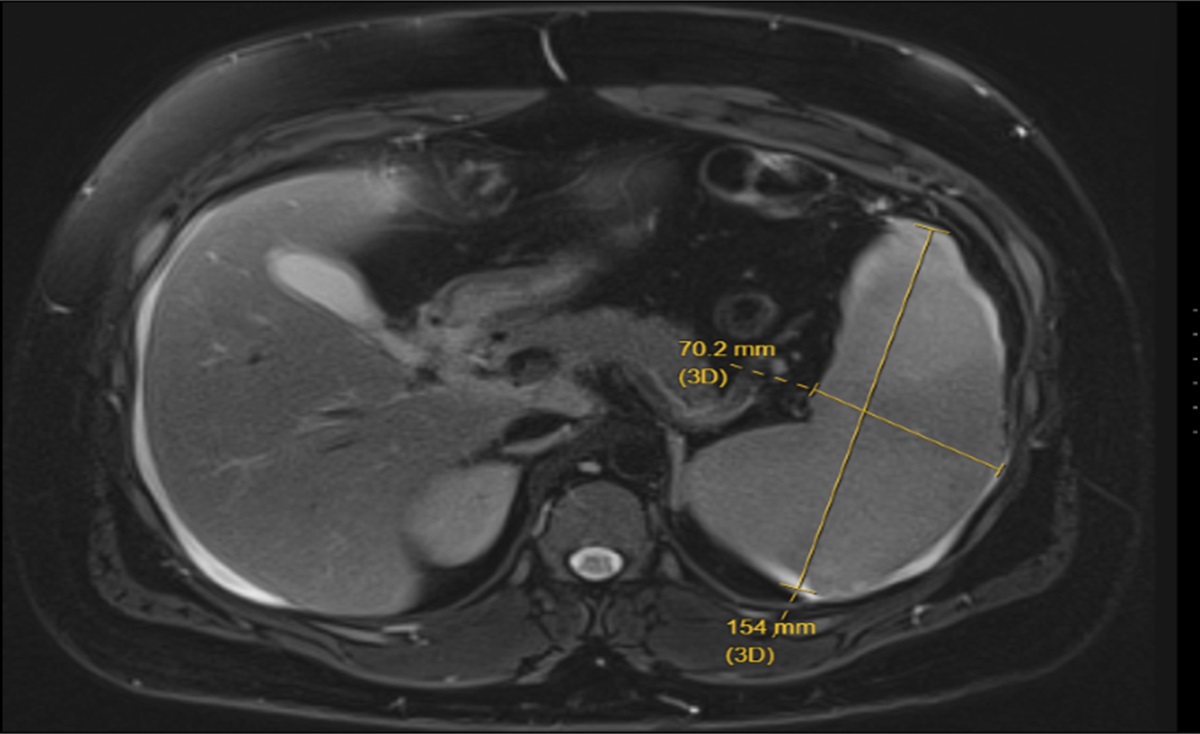
Magnetic resonance imaging of the rectum demonstrated vascular engorgement and heterogeneous enhancement, consistent with active inflammation/colitis in addition to a primary 4.9 × 5.9 × 4.1 cm polypoid T3a tumor with a superior rectal lymph node, although none of the biopsies confirmed carcinoma (Figure 2).
 Figure 2.:
Figure 2.: Magnetic resonance imaging of mass in (A) sagittal and (B) coronal views. Size of mass: 4.9 × 5.9 × 4.1 cm (Craniocaudal × Anteroposteior × Transverse).
The patient underwent a proctocolectomy with ileal pouch-anal anastomosis and diverting loop ileostomy. Owing to the presence of dysplasia in the rectum, a mucosectomy and handsewn anastomosis was performed. The colectomy revealed numerous hamartomatous polyps, the largest polyp measuring 6.5 × 4.3 × 4.0 cm with pathology revealing varying low-grade and focal high-grade dysplasia (Figure 3). Immunohistochemical stain was positive for desmin and P53 null expression. Given the absence of carcinoma in the rectum, a loop ileostomy reversal was planned.
 Figure 3.:
Figure 3.: (A) Gross specimen with yellow arrows pointing at numerous tan-brown, pedunculated, and sessile polyps located diffusely throughout the colonic mucosa, with largest a 6.5 × 4.3 × 4.0 cm polypoid mass within the rectum, 1.5 cm from the distal margin. (B) High power (40×) of focal high-grade dysplasia. (C) Low power (4×) of the largest polyp with vascular core.
DISCUSSIONJuvenile polyps may be pedunculated or sessile, containing dilated crypts filled with mucus, neutrophils, and a lamina propria with edema and inflammatory cells with surface erosions. These structural abnormalities lead to gastrointestinal bleeding and resultant anemia.10
Both inflammatory bowel disease (IBD) and JPS can present with anemia, fever, abdominal pain, diarrhea, and hematochezia. Histologically, inflammatory polyps and pseudopolyps, seen more frequently in IBD, can have granulation tissue-like stroma, which makes it difficult to distinguish from juvenile polyps.11
Although solitary juvenile polyps have low malignant potential, patients with JPS carry an increased lifetime risk of 50% of multiple types of gastrointestinal cancer.4
To our knowledge, there have only been 3 case reports discussing simultaneous IBD and JPS.12,13 Although several cases describe UC with solitary juvenile polyps, there are no direct associations between juvenile polyps and IBD.11,14
UC cells release reactive oxygen and nitrogen species, resulting in DNA damage and inaccuracies in intrinsic repairs of coding and regulatory genetic sequences.15 One proposed mechanism of cancer pathogenesis in JPS is the landscaper mechanism, which postulates that genetic alterations at the chromosomal level results in cancer as a result of an abnormal stroma environment.16
The average median age of CRC in JPS is reported at the age of 41 years,17 yet our patient aged 27 years exhibited evidence of focal high-grade dysplasia. We initially hypothesized that the inflammation from uncontrolled UC was contributory to the high-grade dysplasia; however, not only was there limited inflammation observed on direct visualization, but mucosal biopsies from the left colon and rectum also revealed only hyperplastic change in the absence of inflammation. Biopsies of the polyps themselves were juvenile and inflammatory histologically. This is likely also true for the CT findings after discharge describing left-sided colitis; the inflammatory burden that was observed on imaging was secondary to wall thickening from significant polyposis burden rather than inflammatory colitis.
Nevertheless, further investigation is needed to determine if IBD can alter the regulatory genes of these hamartomatous polyps, leading to an accelerated progression to malignancy. The increased cancer risk in JPS may require shorter time intervals of surveillance and anti-inflammatory therapy.
DISCLOSURESAuthor contributions: T. She, S. Ren, and S. Katz made substantial contributions to the conception or design of the work and interpretation of data for the work. T. She drafted the work, revising it critically for important intellectual content along with the help of S. Ren, H. He and M. Symer. Images created by T. She. All Authors reviewed all content and made several revisions and edits for intellectual and grammar content. S. Katz is the article guarantor. Final approval of the version to be published was reviewed by all authors.
Acknowledgments: Jianhong Zhou, MD, and the Department of Pathology.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
REFERENCES 1. Aretz S, Stienen D, Uhlhaas S, et al. High proportion of large genomic deletions and a genotype phenotype update in 80 unrelated families with juvenile polyposis syndrome. J Med Genet. 2007;44(11):702–9. 2. Jass JR, Williams CB, Bussey HJ, Morson BC. Juvenile polyposis—A precancerous condition. Histopathology. 1988;13(6):619–30. 3. Chow E, Macrae F. A review of juvenile polyposis syndrome. J Gastroenterol Hepatol. 2005;20(11):1634–40. 4. Lutgens MW, van Oijen MG, van der Heijden GJ, Vleggaar FP, Siersema PD, Oldenburg B. Declining risk of colorectal cancer in inflammatory bowel disease: An updated meta-analysis of population-based cohort studies. Inflamm Bowel Dis. 2013;19(4):789–99. 5. Flores BM, O'Connor A, Moss AC. Impact of mucosal inflammation on risk of colorectal neoplasia in patients with ulcerative colitis: A systematic review and meta-analysis. Gastrointest Endosc. 2017;86(6):1006–11.e8. 6. Brosens LA, van Hattem A, Hylind LM, et al. Risk of colorectal cancer in juvenile polyposis. Gut. 2007;56(7):965–7. 7. Campos FG, Figueiredo MN, Martinez CA. Colorectal cancer risk in hamartomatous polyposis syndromes. World J Gastrointest Surg. 2015;7(3):25–32. 8. Jess T, Rungoe C, Peyrin-Biroulet L. Risk of colorectal cancer in patients with ulcerative colitis: A meta-analysis of population-based cohort studies. Clin Gastroenterol Hepatol. 2012;10(6):639–45. 9. Rutter MD, Saunders BP, Wilkinson KH, et al. Thirty-year analysis of a colonoscopic surveillance program for neoplasia in ulcerative colitis. Gastroenterology. 2006;130(4):1030–8. 10. Rosty C. The role of the surgical pathologist in the diagnosis of gastrointestinal polyposis syndromes. Adv Anat Pathol. 2018;25(1):1–13. 11. Chen YW, Tu JF, Shen WJ, Chen WY, Dong J. Diagnosis and management of a solitary colorectal juvenile polyp in an adult during follow-up for ulcerative colitis: A case report. World J Gastroenterol. 2020;26(8):877–82. 12. Faisal MS, Cruise M, Burke CA, et al. S3382 juvenile polyposis syndrome & inflammatory bowel disease: Balancing the risk of malignancy. Am J Gastroenterol. 2020;115(1):S1758. 13. Elhjouji A, Aitali A, Rouibaa F, Rharrassi I, Zentar A, Sair K. Colorectal juvenile polyposis in an adult with ulcerative colitis. J Visc Surg. 2011;148(1):64–6. 14. Nugent KP, Talbot IC, Hodgson SV, Phillips RK. Solitary juvenile polyps: Not a marker for subsequent malignancy. Gastroenterology. 1993;105(3):698–700. 15. Li W, Zhao T, Wu D, et al. Colorectal cancer in ulcerative colitis: Mechanisms, surveillance and chemoprevention. Curr Oncol. 2022;29(9):6091–114. 16. Brosens LA, Langeveld D, van Hattem WA, Giardiello FM, Offerhaus GJA. Juvenile polyposis syndrome. World J Gastroenterol. 2011;17(44):4839–44. 17. Blatter R, Tschupp B, Aretz S, et al. Disease expression in juvenile polyposis syndrome: A retrospective survey on a cohort of 221 European patients and comparison with a literature-derived cohort of 473 SMAD4/BMPR1A pathogenic variant carriers. Genet Med. 2020;22(9):1524–32.
Comments (0)