
Remember me





Multiple myeloma (MM) is a malignancy characterized by the uncontrolled growth of plasma cells in the bone marrow. This uncontrolled growth disrupts normal hematopoiesis, and the most common symptoms of MM stem from the disruption of hematopoiesis resulting in anemia. Other symptoms of MM include bone pain, bone aches, fatigue, hypercalcemia, and kidney failure.1 Gastrointestinal (GI) symptoms are extraordinarily rare.
A plasmacytoma is an abnormal collection of plasma cells that is a solitary tumor, usually within bone, but can also found in extramedullary soft tissue. Plasmacytomas can also be associated with MM and are then considered extramedullary myelomas (EMM). The mechanism of MM cells disseminating to extramedullary sites is not well understood; however, proposed mechanisms involve the microenvironment between the MM cells and the bone marrow.2,3 The alteration in the expression of chemokine receptors and adhesion molecules on MM cells possibly leads to dissemination from the bone marrow into the extramedullary environment.2 In addition, Handa et al discovered long noncoding RNAs regulating gene expression, specifically MALAT1, are found in higher quantities in extramedullary MM cells compared with intramedullary MM cells.4 In patients with MM, EMM is defined as plasma cells found outside of the bone marrow in distant soft-tissue sites. EMM at the time of diagnosis of MM is extremely rare and is associated with a poor prognosis. EMM, however, can occur in up to 30% of patients throughout the disease course of MM. The most common sites for spread include the liver, kidney, central nervous system, and lymph nodes.5 Extramedullary GI plasmacytomas are exceedingly rare, accounting for only 4% of all plasmacytomas.6
CASE REPORTAn 83-year-old man presented to the hospital with a 2-month history of fatigue, dyspnea on exertion, and melena. His medical history was significant for chronic anticoagulation therapy, coronary artery disease, and chronic kidney disease. Vital signs were significant for a heart rate of 112 beats per minute and normal blood pressure. His physical examination was remarkable for a chronically ill-appearing male individual, with irregularly irregular heart rhythm, and scattered bruises on bilateral upper extremities. Rectal examination revealed melena.
Two months before his presentation, the patient's laboratory test results were significant for a hemoglobin of 12.2 g/dL. His creatinine had recently increased from his previous baseline of 1.2–1.57 mg/dL, and his calcium was normal at 9.1 mg/dL. At the time of his presentation, his laboratory test results were significant for a hemoglobin of 7.6 g/dL, a platelet count of 112 103/×μL, a corrected calcium of 11.6 mg/mL, and a creatinine of 5.37 mg/dL. He underwent an abdominal and pelvic computed tomography imaging, which was significant for a mass-like soft-tissue density in his pelvis.
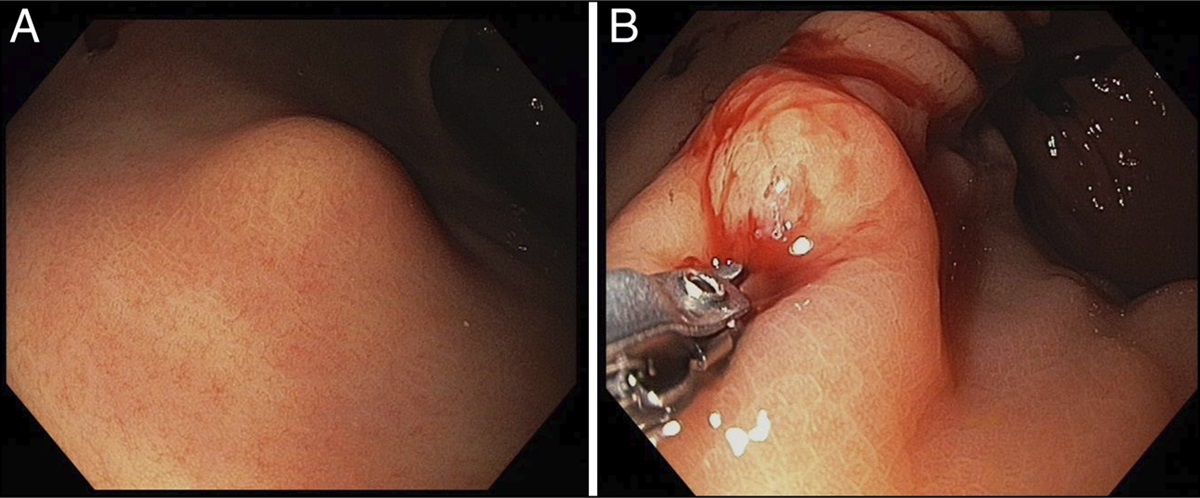
Because of the complaint of melena and concern for GI bleeding, the patient had an upper endoscopy, which revealed 3 bleeding 4–7 mm umbilicated papules in the proximal stomach, seen in Figure 1. Biopsies were taken, and the pathology showed a diffuse mucosal infiltrate of atypical, anaplastic plasma cells with multinucleation, nucleoli, and numerous mitotic figures, as shown in Figure 2. The plasma cells were kappa restricted by kappa/lambda in situ hybridization, displayed in Figure 3. These findings were consistent with extramedullary plasmacytomas, and the clinical picture overall was concerning for a new diagnosis of MM.
 Figure 1.:
Figure 1.: Retroflexion view during upper endoscopy demonstrating actively bleeding extramedullary gastric myeloma.
 Figure 2.:
Figure 2.: Hematoxylin and eosin stain of the gastric nodule biopsy at 400× magnification showing anaplastic and atypical plasma cells with multinucleation, nucleoli, and numerous mitotic figures.
 Figure 3.:
Figure 3.: Kappa in situ hybridization at 100× magnification showing the plasma cells are kappa-restricted.
Subsequently, a bone marrow biopsy was performed, and it showed numerous neoplastic plasma cells, representing 80% of marrow cellularity. Cytogenetics studies showed a complex hyperdiploid karyotype. These findings were diagnostic of MM.
Because of the patient's age, comorbidities, and severe renal failure, he was a poor candidate for a hematopoietic transplant, so the patient was started on bortezomib, daratumumab, and dexamethasone. This aggressive combination including a proteosome inhibitor, monoclonal antibody, and steroids was chosen because of his MM presenting with significant cancer burden. Lenalidomide, an immunomodulator, was planned to be initiated outpatient. He also required inpatient dialysis because of malignant hypercalcemia, as well as multiple blood transfusions daily because of ongoing upper gastric bleeding from the plasmacytoma. Although there was a plan to biopsy the new soft-tissue density in the pelvis noted on the computed tomography imaging, the patient opted to transition to comfort measures because of his clinical forecast and the burden of his diagnosis.
DISCUSSIONOur case is an unusual presentation for a new diagnosis of MM exhibiting as a severe upper GI bleed from a gastric plasmacytoma, representing an EMM in the setting of newly diagnosed MM. Only 3.3% of people with MM have extramedullary disease at the time of diagnosis, and presentation with extramedullary disease is associated with a worse prognosis.7 Plasma cell neoplasms involving the GI tract are rare, and bleeding GI lesions are even more uncommon, with 1 literature review documenting only 27 such case reports of this presentation. In 25% of those cases, the patient later went on to be diagnosed with MM. Melena was the main presenting complaint in almost half of those of those patients.8
This case contributes to the existing body of literature by describing a patient with fatigue and dyspnea with active GI bleeding from gastric nodules initially believed to be isolated extramedullary plasmacytomas. After a bone marrow biopsy confirmed MM, the plasma cell neoplasms were discovered to be extramedullary gastric myeloma, a rare sequela of the patient's new MM diagnosis.
The presence of extramedullary disease in a patient with MM is a poor prognostic sign, and aggressive treatment is recommended.5 Although treatment is not standardized, a combination approach consisting of a proteasome inhibitor, immunomodulatory agents, and steroids is considered key treatment.9 Bortezomib, a proteasome inhibitor, has shown promise in improving outcomes of extramedullary disease and is considered a valuable component when treating aggressive manifestations of MM.9,10 Autologous stem cell transplants are the preferred treatment progression after initial treatment in eligible patients.5,10
In conclusion, we highlight the importance of early GI intervention in a patient with upper GI bleeding because of the poor prognostic factors associated with EMM in patients with MM. Although gastric plasmacytomas are a rare cause of GI bleeding, they have implications for aggressive treatment and should remain on the differential of acute upper GI bleeds. Swift diagnosis through tissue biopsy was crucial to diagnosing this gastric plasmacytoma, ultimately leading to our patient's diagnosis of MM.
DISCLOSURESAuthor contributions: KH Shepherd and M. Willard: performed the literature review, wrote and edited the manuscript. G. Obeng: developed the concept and wrote and edited the manuscript. J. Kolodney: contributed to the oncology portion of the manuscript and edited the final manuscript. C. Randall: acquired pathology images as well as contributing to the pathology discussion in the manuscript. KH Shepherd is the article guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
REFERENCES 1. Ramsenthaler C, Kane P, Gao W, et al. Prevalence of symptoms in patients with multiple myeloma: A systematic review and meta-analysis. Eur J Haematol. 2016;97(5):416–29. 2. Bladé J, de Larrea CF, Rosiñol L. Extramedullary involvement in multiple myeloma. Haematologica. 2012;97(11):1618–9. 3. Bansal R, Rakshit S, Kumar S. Extramedullary disease in multiple myeloma. Blood Cancer J. 2021;11(9):161. 4. Handa H, Kuroda Y, Kimura K, et al. Long non-coding RNA MALAT1 is an inducible stress response gene associated with extramedullary spread and poor prognosis of multiple myeloma. Br J Haematol. 2017;179(3):449–60. 5. Touzeau C, Moreau P. How I treat extramedullary myeloma. Blood. 2016;127(8):971–6. 6. Glasbey JC, Arshad F, Almond LM, et al. Gastrointestinal manifestations of extramedullary plasmacytoma: A narrative review and illustrative case reports. Ann R Coll Surg Engl. 2018;100(5):371–6. 7. Cowan AJ, Green DJ, Kwok M, et al. Diagnosis and management of multiple myeloma: A review. JAMA. 2022;327(5):464–77. 8. Iosif E, Rees C, Beeslaar S, Shamali A, Lauro R, Kyriakides C. Gastrointestinal bleeding as initial presentation of extramedullary plasma cell neoplasms: A case report and review of the literature. World J Gastrointest Endosc. 2019;11(4):308–21. 9. Li Y, Sun Z, Qu X. Advances in the treatment of extramedullary disease in multiple myeloma. Transl Oncol. 2022;22:101465. 10. Li G, Song YP, Lv Y, Li ZZ, Zheng YH. Clinical characteristics and prognostic analysis of multiple myeloma with extramedullary disease: A SEER-based study. J Oncol. 2021;2021:6681521–9.
Comments (0)