
Remember me





Atraumatic splenic rupture (ASR), a potentially life-threatening complication, is an infrequent yet critical manifestation of infectious mononucleosis (IM), commonly caused by the Epstein-Barr virus (EBV). It is widely reported that EBV infects over 90% of the population, but of those infected, most remain asymptomatic.1 While splenomegaly may not always be palpable, ultrasound evaluations consistently show varying degrees of splenic enlargement in all patients with acute IM.2,3 Although all develop splenomegaly, the incidence of ASR has been documented in only 0.1%–0.5% of cases.3
We present a case of EBV infection masquerading as cholangitis that evolved into spontaneous splenic rupture. Understanding the broad presentation of ASR is crucial for timely recognition and appropriate intervention.
CASE REPORTA 26-year-old man with no medical history presented with sharp epigastric and periumbilical pain worsening over 1 week. He also reported 1 week of malaise, subjective fevers, headache, vomiting, and dark urine.
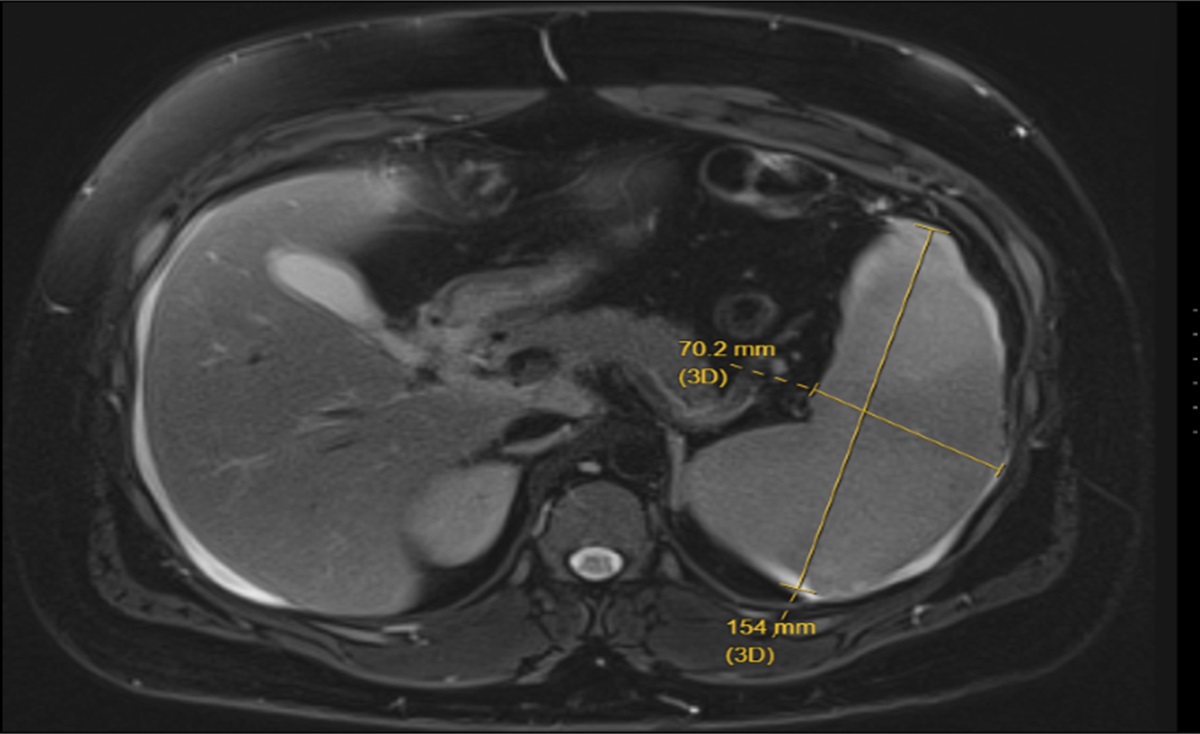
On the initial evaluation, he was tachycardic and febrile to 101.1°F. White blood cell count was 6.85 × 103 μL with a lymphocytosis of 4.25×103 μL. Total bilirubin was elevated to 3.8 mg/dL, alanine transaminase (ALT) 215 U/L, aspartate aminotransferase (AST) 245 U/L, alkaline phosphatase 217 U/L, lactate 2.3 mmol/L, and hepatitis A immunoglobulin M (IgM) was positive. Additional investigations for acute liver injury including hepatitis B, hepatitis C, acetaminophen, and plasma ethanol levels were all within normal limits. A right upper quadrant ultrasound was significant for gallbladder sludge, pericholecystic fluid, thickened gallbladder wall, and mild common bile duct dilation to 5 mm. He was admitted with concerns about acute cholecystitis vs acute cholangitis. He received 3 L of intravenous fluids, was started on piperacillin-tazobactam, and underwent magnetic resonance cholangiopancreatography (MRCP). MRCP revealed splenomegaly, splenic infarcts, and a nondilated biliary tree without evidence of cholangitis or acute cholecystitis (Figure 1).
 Figure 1.:
Figure 1.: Magnetic resonance cholangiopancreatography demonstrating splenomegaly, the spleen measures 154 mm in length.
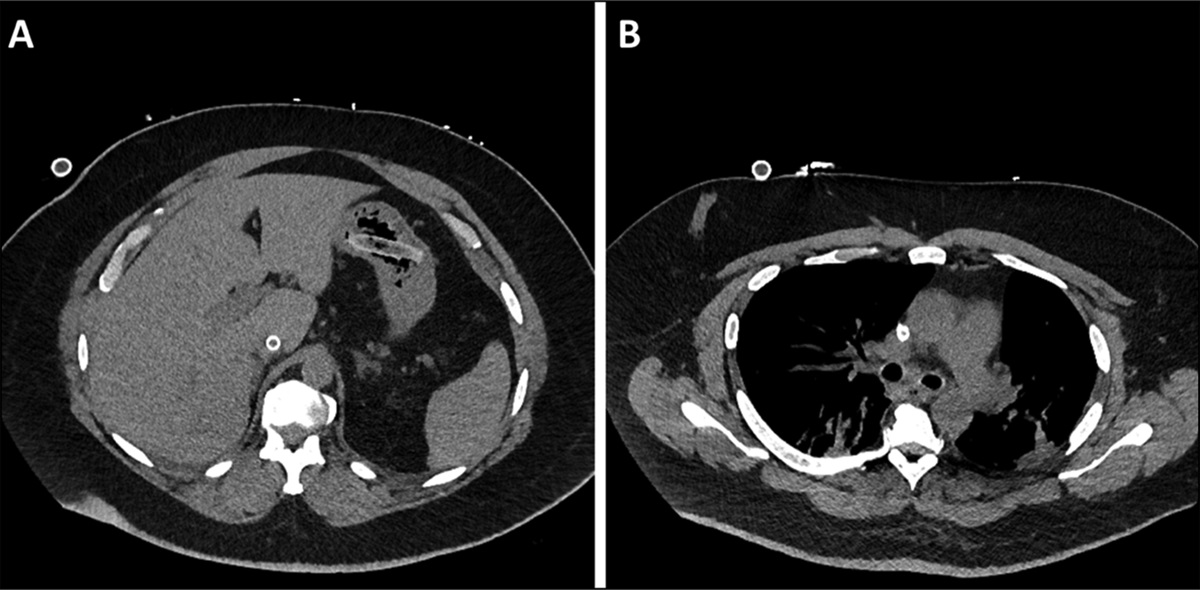
Overnight, he became diaphoretic, febrile to 102.3 F, and hypotensive despite 4 L of intravenous fluids. An abdominal computed tomography angiography scan 12 hours after MRCP revealed a ruptured spleen with hemoperitoneum (Figure 2). He was emergently taken to the operating room for successful splenectomy and subsequent cholecystectomy that revealed an inflamed gallbladder. EBV titers and viral load collected at that time were positive for EBV IGM >160 μ/mL and EBV DNA 306,635 IU/mL. His liver enzymes downtrended throughout hospitalization and normalized 2 months later. He was vaccinated against Streptococcus pneumoniae, Haemophilus influenzae type b, and Neisseria meningitidis before discharge.
 Figure 2.:
Figure 2.: Abdominal computed tomography angiography scan revealing ruptured spleen with hemoperitoneum.
DISCUSSIONIM, mostly caused by EBV, is a lymphoproliferative disorder primarily transmitted through saliva.4 Some reports estimate that EBV infects over 90% of the population, but most remain asymptomatic.1 EBV predominantly becomes symptomatic in young adults and classically presents as IM characterized by a prolonged course of fever, exudative pharyngitis, fatigue, and tender lymphadenopathy.4 The best initial diagnostic test for EBV is the heterophile antibody test with a sensitivity of 63%–84% and specificity of 84%–100%.3 However, the heterophile antibody titer can take 2–5 weeks to peak, so a negative test cannot always exclude the diagnosis.3 During the acute phase, the EBV viral capsid antigen IgM antibody test can be of diagnostic value.3
Standard management for IM is supportive care with rest, analgesia, and hydration. Although not always palpable, ultrasound has detected splenomegaly in 100% of confirmed cases.2,3 Complications such as splenic rupture can occur but have only been reported in 0.1%–0.5% of cases.3 The pathophysiology of splenic rupture is believed to be secondary lymphocytic infiltration stretching the splenic capsule and increasing splenic fragility.2 Splenomegaly can also reduce protection by the rib cage, thus predisposing patients to splenic injury.2 Although splenic rupture most commonly occurs secondary to trauma, in rare cases, like the one we present above, ASR can occur. A study by Liu et al retrospectively identified 251 patients with splenic rupture and only 3.2% or 8 patients were found to have ASR.5 Common risk factors of ASR include infection, neoplastic and inflammatory disorders, and congestive splenomegaly.5 A systematic review of 85 cases involving splenic rupture specifically in patients with IM reported all ruptures occurred within 4 weeks of symptom onset, 88% presented with acute abdominal pain, 70% occurred in male patients, the average age was 22 years, and a history of trauma was reported in only 14% of cases.2
Diagnosing ASR can present a challenge; however, the use of physical examination, laboratory findings, and imaging aid in diagnosis. Vitals may reveal tachycardia and hypotension secondary to hypovolemic shock. Examination findings commonly include abdominal pain, splenomegaly, and Kehr sign. Kehr sign, described as left shoulder pain resulting from diaphragmatic irritation from hemoperitoneum, has been reported in approximately 50% of splenic rupture cases.1,2 Laboratory findings may reveal anemia and lymphocytosis. Elevated liver function tests have been found in 75% of cases.3 Abdominal computed tomography is the preferred method of imaging in hemodynamically stable patients with a sensitivity of 85.7%, and specificity of 100%.5,6 Computed tomography findings that aid in diagnosis are hemoperitoneum or contrast extravasation, lacerations, splenic hypodensity, and subcapsular or intraparenchymal hematomas.7 If splenic rupture is confirmed, the initial management depends on hemodynamic status, etiology of rupture, and splenic injury grade.8 Current guidelines recommend considering nonoperative management for hemodynamically stable patients, while splenectomy is the choice of treatment for hemodynamically unstable patients.9 Since asplenic patients are at risk of invasive infections, particularly with encapsulated bacteria, it is recommended that patients be vaccinated against Streptococcus pneumoniae, Haemophilus influenzae type b, and Neisseria meningitidis within 2 weeks of emergent splenectomy.10
In this case, the initial clinical picture was complicated by symptoms, laboratory results, and imaging supporting the diagnosis of acute cholecystitis or cholangitis in which MRCP ruled out. Although rare, EBV has been documented to cause cholestatic hepatitis, which could be the etiology of our patient's initial clinical picture.11 Early diagnostic clues in our case that pointed further to EBV were his age and symptoms of prolonged malaise, lymphocytosis, and splenomegaly. Overall, ASR is a rare complication of IM; however, it is the deadliest with a mortality of 9%–12.2%.2,8 This highlights the importance of promptly diagnosing IM and understanding the broad presentation and warning signs of splenic rupture for timely recognition and appropriate intervention.
DISCLOSURESH. Darnell, S. Bidarian, A. Brenner, and J. Auer contributed equally by reviewing literature, providing images, and drafting and revising the final manuscript. J. Auer is the article guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
REFERENCES 1. Baker CR, Kona S. Spontaneous splenic rupture in a patient with infectious mononucleosis. BMJ Case Rep. 2019;12(9):e230259. 2. Bartlett A, Williams R, Hilton M. Splenic rupture in infectious mononucleosis: A systematic review of published case reports. Injury. 2016;47(3):531–8. 3. Fugl A, Andersen CL. Epstein-Barr virus and its association with disease: A review of relevance to general practice. BMC Fam Pract. 2019;20(1):62. 4. Sylvester JE, Buchanan BK, Silva TW. Infectious mononucleosis: Rapid evidence review. Am Fam Physician. 2023;107(1):71–8. 5. Liu J, Feng Y, Li A, Liu C, Li F. Diagnosis and treatment of atraumatic splenic rupture: Experience of 8 cases. Gastroenterol Res Pract. 2019;2019:5827694. 6. Sortland O, Nerdrum HJ, Solheim K. Computed tomography and scintigraphy in the diagnosis of splenic injury. Acta Chir Scand. 1986;152:453–61. 7. Sergent SR, Johnson SM, Ashurst J, Johnston G. Epstein-Barr virus-associated atraumatic spleen laceration presenting with neck and shoulder pain. Am J Case Rep. 2015;16:774–7. 8. Renzulli P, Hostettler A, Schoepfer AM, Gloor B, Candinas D. Systematic review of atraumatic splenic rupture. Br J Surg. 2009;96(10):1114–21. 9. Scarborough JE, Ingraham AM, Liepert AE, Jung HS, O'Rourke AP, Agarwal SK. Nonoperative management is as effective as immediate splenectomy for adult patients with high-grade blunt splenic injury. J Am Coll Surg. 2016;223(2):249–58. 10. Bonanni P, Grazzini M, Niccolai G, et al. Recommended vaccinations for asplenic and hyposplenic adult patients. Hum Vaccin Immunother. 2017;13(2):359–68. 11. Da Cunha T, Mago S, Bath RK. Epstein-Barr virus reactivation causing cholestatic hepatitis. Cureus. 2022;14(4):e24552.
Comments (0)