
Remember me





We present a case of a 67-year-old patient with an incidental finding of a submucosal lesion in the gastric antrum in the esophagogastroduodenoscopy. The decision to perform an endoscopic resection was made due to a low-grade growth on follow-up. Owing to the borderline size, we performed a hybrid resection technique (endoscopic full-thickness resection [EFTR] and endoscopic submucosal dissection [ESD] combined). This technique is already being used for submucosal lesions in the lower gastrointestinal (GI) tract but has not yet been frequently applied in the upper GI tract. Data concerning safety and efficacy of this technique are scarce. To our surprise, the submucosal tumor later turned out to be a schwannoma.
CASE REPORTA 67-year-old man was referred for an upper and lower panendoscopy due to a severe iron-deficiency anemia with hemoglobin of 63 g/L and ferritin of 4.8 μg/L. He originally consulted his general practitioner due to progressive fatigue and paleness. The patient noticed hematochezia, and there were no night sweats, fever, or unintentional weight loss. His personal medical history was otherwise nonsignificant, and there was no positive family history of colorectal cancer or inflammatory bowel disease. His last colonoscopy 10 years ago did not show any pathological findings. His vital signs were normal, and he was slightly overweight with a body mass index of 27 kg/m2. As a long-term medication, he was taking escitalopram 10 mg, finasteride 1 mg, and pantoprazole 40 mg twice daily.
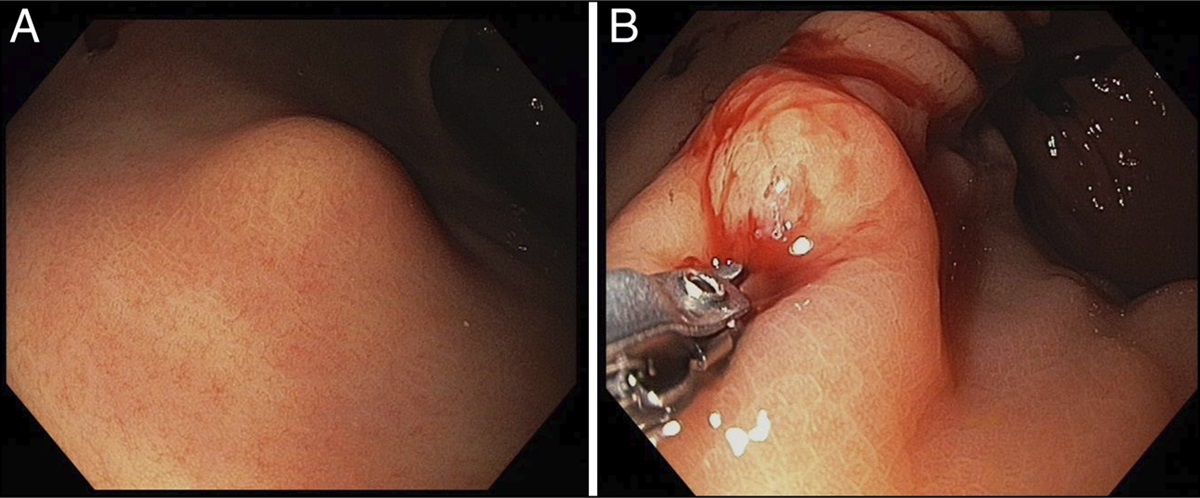
In the initial upper GI endoscopy, we found no source of upper GI bleeding, particularly no malignant lesions. As an incidental finding, we discovered a submucosal lesion in the gastric antrum (Figure 1). Buttonhole biopsies were taken and were inconclusive (Figure 1).
 Figure 1.:
Figure 1.: (A) Shows the initial endoscopic picture of the submucosal lesion. (B) Shows the bite-on-bite biopsy, which was unrevealing.
The colonoscopy showed a mild sigma diverticulosis and second-degree haemorrhoids as a potential source of the lower GI bleeding, and rubber band ligations were applied. Upper endoscopic ultrasound (EUS) was performed to further assess the submucosal lesion of the gastric antrum, which showed a homogenous, hypoechoic, 11 × 8 mm lesion, originating from the muscularis propria with a sharp border (Figure 2). There were no perifocal lymph nodes. Assuming a low-risk GI stromal tumor (GIST), we recommended yearly gastroscopic and endosonographic follow-up, as there is no compelling indication for surgery in a GIST smaller than 2 cm. We decided against EUS-guided biopsy because of the absence of high-risk features and the small tumor size.
 Figure 2.:
Figure 2.: Endoscopic ultrasound, showing (A) the initial picture of the submucosal lesion with 11 mm diameter and (B) the tumor growth to a diameter of 14 mm.
After 6 years, there was a progression to 14 × 8 mm (Figure 2). Since the patient was concerned about potential malignancy, we discussed the therapeutic options offering further follow-up and surgical or endoscopic resection. The patient decided for endoscopic resection due to the less invasive character of the intervention. The planned EFTR was performed under intubation anesthesia. Considering the size of the lesion, which would not allow a safe R0-resection by EFTR alone, a combined ESD and EFTR (hybrid ESD-EFTR) was performed. Initially, the lesion was incised circumferentially with a triangle tip knife after submucosal injection of physiogel with adrenaline 1:100,000 and indigo carmine. With this technique, the amount of mucosal tissue was reduced, allowing to completely pull the lesion into the cap of the full-thickness resection device to reach a safe and macroscopically complete resection (Figure 3).
At second-look gastroscopy on the following day, a double clip application was performed and Nexpowder was applied in the area of the resection site due to persistent bleeding. There was no significant postinterventional decrease in hemoglobin (120–117 g/L) why the patient was discharged after 2 nights. Contrary to expectations, histology revealed a schwannoma, histologically completely resected (Figure 4).
 Figure 3.:
Figure 3.: Hybrid ESD/EFTR showing (A) the endoscopic incision with the needle-knife, (B) the circumcised lesion after incision, (C) the lesion after incision and injection of adrenalin and indigo carmine, (D) the uncovered lesion after endoscopic submucosal dissection of the borders of the lesion, (E) postinterventional endoscopic picture with the over-the-scope clip after EFTR, (F) the resected tumor pinned with needles for display, and (G) the mucosal scar 3 months after intervention. EFTR, endoscopic full-thickness resection; ESD, endoscopic submucosal dissection.
 Figure 4.:
Figure 4.: Histology showing (A1) the overview of the tumor in hematoxylin-eosin (HE) staining. (A2) 10-fold magnification of the tumor in HE staining. (B1) the overview of the tumor in the S100 staining. (B2) the 10-fold magnification of the tumor in the S100 staining.
DISCUSSIONSubmucosal lesions in the stomach are often found incidentally during gastroscopy. They are a diagnostic challenge since they can be benign or potentially malignant.
EUS characterizes the lesion and defines the layer of origin. EUS-fine-needle biopsy or mucosal incision-assisted biopsy can be performed to get a histological diagnosis which can be a challenge, especially in smaller lesions.1
GISTs are the most common subepithelial lesions in the gastrointestinal tract with malignant potential usually arising from the proper muscle layer.2
GISTs up to a size of 2 cm can be monitored. GISTs with a size of more than 2 cm should always be resected, due to the malignant potential.3
Whether resection is performed endoscopically or surgically is an individual interdisciplinary decision and mainly depends on the size of the lesions, due to the size of the cap of the full-thickness resection device (FTRD).
The malignant potential of GISTs depends on the mitotic index and the tumor size. Endoscopic ultrasound may help to detect high-risk features (irregular margins, presence of suspect lymph nodes, heterogeneity).4,5
Schwannomas are tumors of the peripheral nervous system, which arise from the so-called Schwann cells. The diagnosis of a schwannoma is made histologically. EUS findings are unspecific, and there is a high risk of confusion with other subepithelial lesions, especially GISTs. They have no malignant potential and therefore need no treatment as long as they do not cause symptoms.6 In case of inconclusive histology, resection can be performed to provide a definite diagnosis and to appropriately advise the patient regarding treatment and follow-up.
EFTR with the FTRD allows the resection of lesions even originating from the proper muscle layer.
The inner diameter of the cap of the FTRD gastroduodenal of 12.1 mm limits the size of the lesions that can be resected. Recent reviews have shown technical success rate of EFTR up to 93%, R0-resection rate up to 76%, and no serious adverse events or perforations.7 Recently 2 cases of delayed perforation after EFTR in submucosal gastric lesions were reported, both due to clip dislodgement. The complications were managed endoscopically and were assumed to be associated with significant scarring of the lesions.8
ESD has shown higher technical success rates up to 97% and R0-resection rates up to 81% but are associated with a higher rate of complications (eg, bleeding ∼10%, perforation 4.10%).9
In the case of borderline large tumors, a hybrid method combining ESD and EFTR can be used to completely resect a submucosal lesion. ESD reduces the amount of mucosa and submucosa making the lesion accessible to EFTR. This hybrid method may increase the R0-resection rate but could be associated with a higher complication rate, further data are needed.
This method is already used for lesions in the lower GI tract, and according to a literature search in PubMed, such a hybrid resection technique in the upper GI tract has only been performed once before.10
We have shown that the hybrid resection method combining ESD and EFTR is a safe and effective alternative for the resection of subepithelial lesions arising from the proper muscle layer, in the upper GI tract. It can be considered especially in borderline-sized lesions where resection with EFTR alone is not feasible.11
DISCLOSURESAuthor contributions: S. Kormann: main author and is the article guarantor. G. Semadeni: supervision of the endoscopic procedure. M. Weber: histologic analysis of the specimen. S. Brand: supervisor of the scientific research. J. Borovicka: supervision of the endoscopic procedure. R. Frei: main endoscopic operator, revision of the final case report.
Financial disclosure: None to report.
Previous presentation: The poster of the case report has been presented at the annual meeting of the Swiss Society of Gastroenterology; September 14-15, 2023; Interlaken, Switzerland.
Informed consent was obtained for this case report.
REFERENCES 1. Deprez PH, Moons LMG, O'Toole D, et al. Endoscopic management of subepithelial lesions including neuroendocrine neoplasms: European Society of Gastrointestinal Endoscopy (ESGE) guideline. Endoscopy. 2022;54(4):412–29. 2. Akahoshi K, Oya M, Koga T, et al. Current clinical management of gastrointestinal stromal tumor. World J Gastroenterol. 2018;24(26):2806–17. 3. Jacobson BC, Bhatt A, Greer KB, et al. ACG clinical guideline: Diagnosis and management of gastrointestinal subepithelial lesions. Am J Gastroenterol. 2023;118(1):46–58. 4. Seven G, Arici DS, Senturk H. Correlation of endoscopic ultrasonography features with the mitotic index in 2- to 5-cm gastric gastrointestinal stromal tumors. Dig Dis. 2022;40(1):14–22. 5. Kim MN, Kang SJ, Kim SG, et al. Prediction of risk of malignancy of gastrointestinal stromal tumors by endoscopic ultrasonography. Gut Liver. 2013;7(6):642–7. 6. Hu J, Ge N, Wang S, et al. The role of endoscopic ultrasound and endoscopic resection for gastric schwannoma: A case series and literature review. J Transl Int Med. 2019;7(4):149–54. 7. Mueller J, Kuellmer A, Schiemer M, et al. Current status of endoscopic full-thickness resection with the full-thickness resection device. Dig Endosc. 2023;35(2):232–42. 8. Johnson PC, Agnihotri A, Loren DE, et al. Clip dislodgement after full-thickness endoscopic resection device removal of scarred gastric subepithelial lesion leading to delayed perforation. ACG Case Rep J. 2023;10(12):e01214. 9. Dalal I, Andalib I. Advances in endoscopic resection: A review of endoscopic submucosal dissection (ESD), endoscopic full thickness resection (EFTR) and submucosal tunneling endoscopic resection (STER). Transl Gastroenterol Hepatol 2022;7:19. 10. Angajala V, Yung E, Buxbaum J, Sahakian A. Hybrid resection of GI stromal tumor with endoscopic submucosal dissection and the full-thickness resection device. VideoGIE. 2022;8(1):8–10. 11. Andrisani G, Di Matteo FM. Hybrid resection with endoscopic submucosal dissection and full-thickness resection: Could this be a rescue treatment in the presence of severe fibrosis? Dig Liver Dis. 2019; 51:607–9.
Comments (0)