
Remember me





Cytomegalovirus (CMV) is a double-stranded DNA virus that is enveloped and widely prevalent among immunocompromised patients. In the latter, such as transplant recipients and AIDS, it can spread to multiple organs in the body, causing various issues such as colitis, retinitis, esophagitis, encephalitis, and pneumonitis. On the other hand, in immunocompetent hosts, CMV infection is asymptomatic or may present as a self-limited mononucleosis-like syndrome.1 There is limited research available on CMV infection of the gastrointestinal tract among immunocompetent patients. Case reports have described gastrointestinal lesions in immunocompetent patients caused by CMV, such as gastroduodenal erosions, gastric perforation, and protein-losing enteropathy.1,2 However, these do not mention any instances of gastric outlet obstruction. In this article, we report a case of extensive CMV gastroduodenitis that caused gastric outlet obstruction in a 30-year-old immunocompetent woman with no significant medical history who presented to Dr Ruth K. M. Pfau, Civil Hospital Karachi, Pakistan.
CASE REPORTA 30-year-old previously healthy South Asian woman presented to Dr Ruth K. M. Pfau, Civil Hospital Karachi, Sindh, Pakistan, with a 1-month history of vomiting. She described having 4–6 episodes of vomiting per day which were projectile in nature, more than a cup in quantity, and associated with intermittent epigastric abdominal pain. She had postprandial fullness relieved with postmeal vomiting, consisting of recently consumed food. The patient had 2 episodes of coffee ground emesis a few days before admission. The history was significant for undocumented weight loss. The systemic review was unremarkable. She denied alcohol, tobacco, or nonsteroidal anti-inflammatory drugs use. There was no other history of prior illness, surgery, or blood transfusion. The patient was a native of rural Sindh, Karachi, Pakistan, and reported no recent travel history. She denied intravenous (IV) drug use or any recent engagement in sexual activities. Menstrual and obstetric histories were unremarkable.
Vitals on admission included temperature of 98.2°F, blood pressure 80/50 mm Hg, pulse 90 beats/min (regular), respiratory rate 16 breaths/min, and oxygen saturation levels 98% on ambient air. The general physical examination had findings suggestive of anemia and dehydration. Systematic clinical examination was unremarkable. In-hospital laboratory investigations included complete blood count which was significant for hemoglobin 8.3 g/dL (normal female: 12.0–16.0 g/dL) and an elevated C-reactive protein 1.5 mg/dL (normal: less than 0.2 g/dL). Serum electrolytes exhibited decreased sodium 132 mEq/L (normal: 136–146 mEq/L) and potassium 2.8 mEq/L (normal: 3.5–5.0 mEq/L). The liver function test highlighted decreased albumin of 3.0 g/dL (normal: 3.5–5.5 g/dL). Further workup was significant for low iron 20 μg/dL (normal female: 50–170 μg/dL), low total iron-binding capacity 134 μg/dL (normal: 250–400 μg/dL), decreased folate 2 ng/mL (normal: 2.7–17.0 ng/mL), and decreased uric acid 2.0 mg/dL (normal: 3.0–8.2 mg/dL). Urinalysis was unremarkable except for trace proteinuria. Serological tests indicated no recent infection with hepatitis B virus and hepatitis C virus. Serum immunoglobulin levels were unremarkable. Stool antigen for Helicobacter pylori was negative, and serum gastrin level was 18 pg/mL (normal: 13–115 pg/mL).
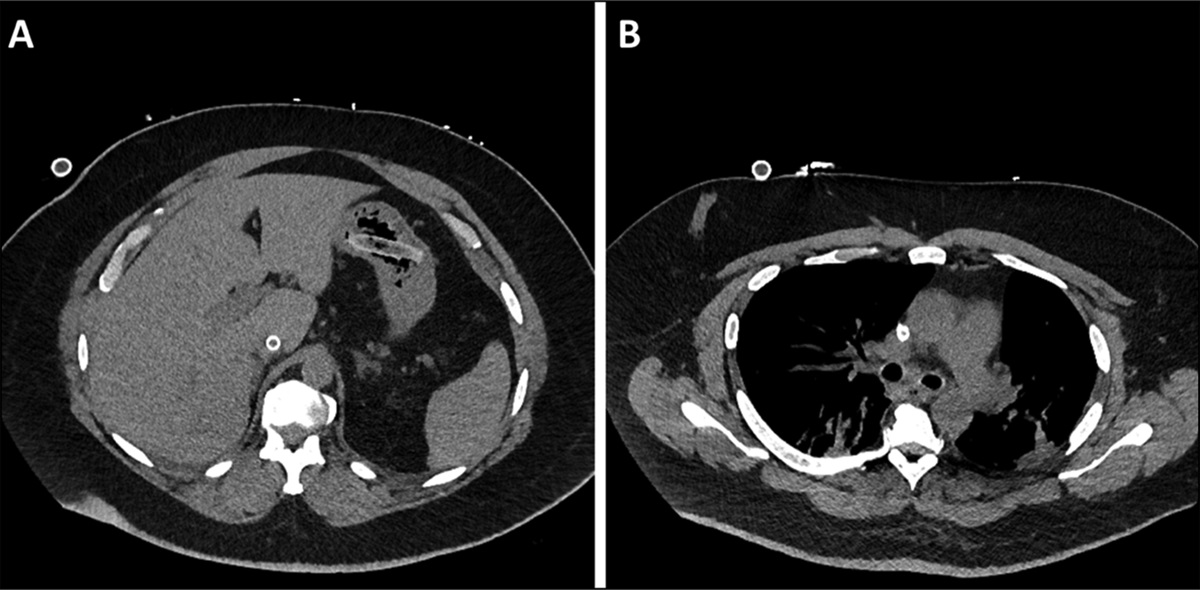
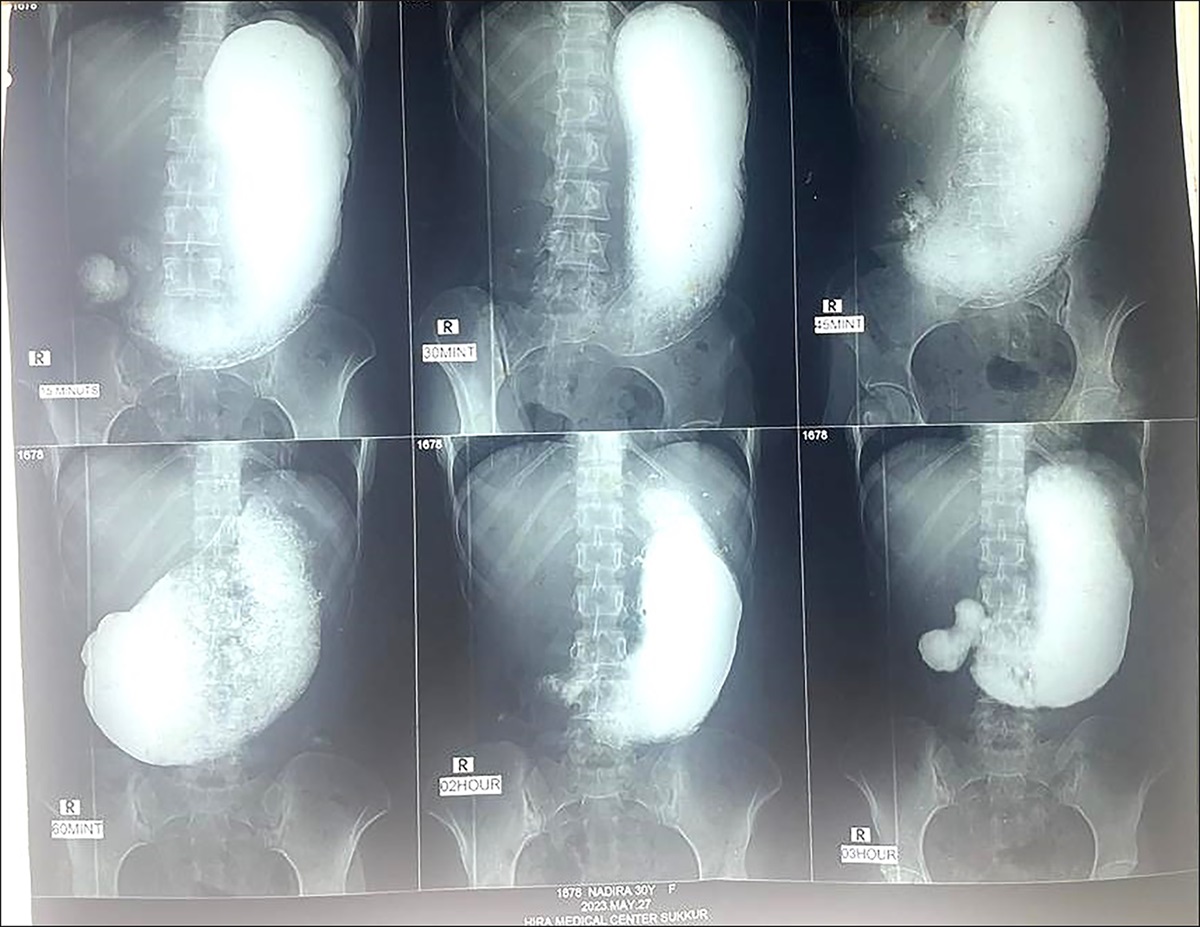
Chest X-ray was unremarkable. Ultrasound scan of the abdomen showed fluid-filled and distended stomach and bowel loops. Barium meal revealed over distended stomach (Figure 1). No gastric emptying was seen even after 2.5 hours of study, suggestive of gastric outlet obstruction. Abdominal computed tomography scan with contrast revealed dilatation of the stomach up to the antrum with circumferential thickening in the pylorus. In contrast to the normal thickness of 2 mm, pylorus single wall thickness measured 10 mm. Moreover, small and large bowel circumferential mural thickening secondary to inflammatory bowel disease was apparent (Figure 2).
 Figure 1.:
Figure 1.: Barium meal showing distended stomach with empty distal duodenum.
 Figure 2.:
Figure 2.: Computed tomography scan showing antral-wall thickening.
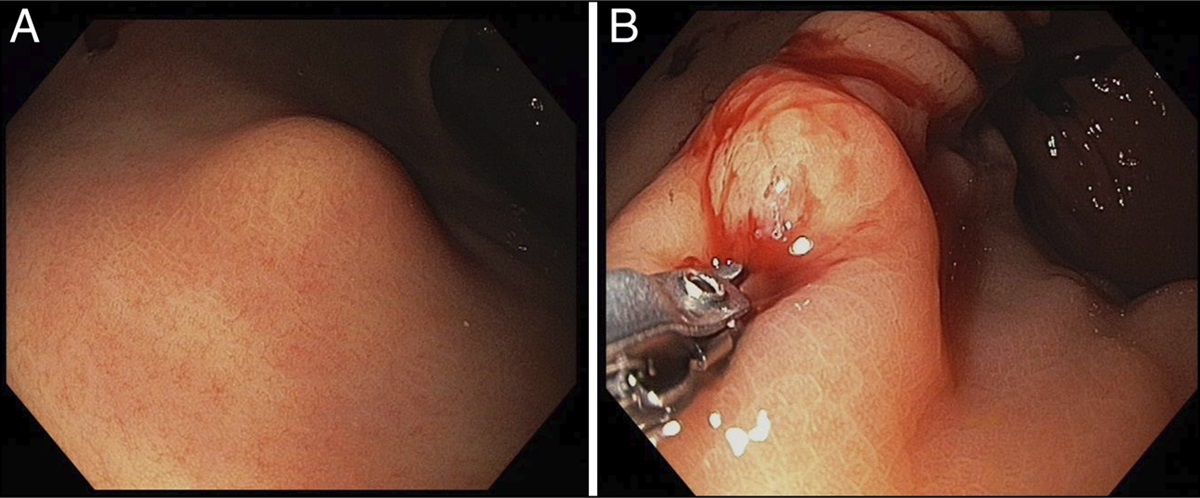
Esophagogastroduodenoscopy (EGD) concluded moderate esophagitis and diffused severe gastritis. In addition, severe antral scaring with mucosal friability, diminished rugal folds, and multiple white-based ulcers extending to the duodenum were also evident. The duodenum bulb appeared inflamed, and scope could not be negotiated in the second part of the duodenum, highlighting duodenal narrowing (Figure 3). Biopsies were obtained from the stomach and duodenum.
 Figure 3.:
Figure 3.: Endoscopy showing the gastric ulcer.
Staining of the gastric biopsy specimens with hematoxylin and eosin revealed ulcer slough with granulation tissue and scattered large cells with intranuclear inclusions, characteristic of CMV infection (Figure 4, left). Immunohistochemistry using monoclonal CMV antibodies was also positive (Figure 4, right). No evidence of granulomas or malignancy was observed. Cytokeratin AE1/AE3 immune stain was negative. CMV infection was further confirmed with positive CMV-DNA polymerase chain reaction and positive serology CMV immunoglobulin M (IgM) 2.57 and immunoglobulin G (IgG) 37.4 (normal < 0.9). A screening HIV test was found to be negative with a CD4 > 500 cells/mm3. Gastric lavage for Tuberculosis Gene Xpert tested negative. Colonoscopy was unremarkable.
 Figure 4.:
Figure 4.: Left, hematoxylin-eosin staining showing cytomegalic inclusions (arrows); right, immunostaining with anticytomegalovirus antibody.
The patient was initiated on a treatment course consisting of oral proton pump inhibitor 40 mg, ganciclovir 250 mg IV twice daily, and nutritional support through nasojejunal tube. Her gastrointestinal and systemic symptoms improved subsequently. Follow-up EGD with biopsy carried out 14 days after the initiation of treatment and was notable for densely inflamed granulation tissue with a lesser number of CMV inclusions. No evidence of malignancy was observed. She completed 2 months of prescribed therapy without any significant adverse or unanticipated events. She was discharged and prescribed nasojejunal tube feeds and IV antibiotics.
Follow-up EGD revealed pinhole opening in the pylorus consistent with pyloric stenosis. This was proceeded with pyloric dilation with controlled radial expansion (CRE) balloon dilatation catheter size 8Fr. The patient was discharged on a clear liquid diet. On the follow-up 2 weeks later, the patient was tolerating a soft diet without any issues. On examination, the stomach appeared normal with no signs of distension or tenderness. In addition, gut sounds were audible. It was recommended that she gradually progress toward an advanced diet.
DISCUSSIONTo date, scarce research is available on CMV gastrointestinal tract infection in immunocompetent adults. Most CMV gastric disease cases in immunocompetent patients are reported in men based on limited available case reports. Isolated CMV gastroduodenitis causing gastric outlet obstruction in an immunocompetent patient has not been reported until now.
Significant variations in disease presentation can be discerned among the abovementioned case reports. To start with, CMV infection is associated with the presence of atypical lymphocytes or reactive lymphocytosis in peripheral blood smears. Our patient presented with a normal total leukocyte count with no evidence of atypical lymphocytes. Beany et al1 report a CMV-related gastric ulcer and gastroduodenitis case in an immunocompetent patient with mild leukocytosis but no atypical lymphocytes. Conversely, Himoto et al noted the presence of atypical lymphocytes in an immunocompetent patient with CMV-associated acute gastric mucosal lesion.3
In addition, Crespo et al report a case of gastritis in an immunocompetent male with an elevated CMV IgM and negative IgG, suggesting primary CMV infection.4 This is in contrast to our present patient who has elevated CMV IgM and IgG, suggesting chronic infection. The latter might explain the severe clinical presentation of gastric outlet obstruction reported in this case compared with superficial erosions in the former.
Claeys et al report coinfection of CMV and H. pylori gastritis.5 Similarly, Crespo et al reported positive immunity to Epstein-Barr virus.4 These data stress testing for association in CMV infection. While being tested negative for H. pylori, our patient was not tested for prior Epstein-Barr virus infection. Despite no change in management, it would have facilitated in comprehending increasing CMV infection in immunocompetent hosts.
While CMV is a well-known pathogen to infect the esophagus and colon among immunocompromised, this case report insinuates the virus's potential to infect any part of the gastrointestinal tract among immunocompetent. In our patient, CMV infection extended beyond the pylorus resulting in duodenal narrowing limiting endoscopic access into the second part of the duodenum. Choi et al report an isolated CMV ileal infection in an immunocompetent male presenting with melena.6 In addition, Monrobel et al report concurrent gastric and colon CMV infection in an immunocompetent female, illustrating the significance of biopsies for ascertaining the etiology of any mucosal lesion.7
Apart from the site of infection, CMV gastrointestinal infection also has variability in the pathophysiology of the disease. Suter et al present a case of CMV-induced transient protein-losing hypertrophic gastropathy mimicking Ménétrier disease.2 The patient presented with massive lower extremity edema, signs of pleural effusion, and a tender abdomen. EGD revealed large rugal folds and chronic erosions in the gastric body and fundus. Laboratory investigations highlighted low albumin 1.76 g/dL (normal: 3.5–5.5 g/dL). In addition, a similar case was reported by Setakhr et al.8 This is in contrast to our patient who had mildly low albumin 3.0 g/dL (normal: 3.5–5.5 g/dL) with diminished rugal folds in the body of the stomach on EGD.
Finally, our patient was treated with proton-pump inhibitors, ganciclovir, and supportive therapy. However, Himoto et al concluded significant clinical and histological improvement without prescribing antivirals.3 Similarly, Beany and Rainis offered supportive therapy coupled with an oral proton-pump inhibitor.1
One of the limitations of the study was the insufficient follow-up, which was primarily due to the participants' inability to afford frequent follow-up visits. This was mainly because the patient resided in a rural area and did not have the financial resources to stay in the city for an extended period, leading to additional travel expenses. Furthermore, due to a lack of consent, an extended family medical history could not be obtained to investigate potential risk factors or modes of transmission of the infection.
This case report sheds light on the different types of presentations of CMV gastrointestinal disease. While it was previously considered primarily a pathogen of the immunosuppressed, there is now an increasing incidence of CMV among the immunocompetent population. This report emphasizes the importance of gastric biopsies in accurately determining the various causes of acute gastric lesions. Furthermore, since there are various modifications of management prescribed in the abovementioned cases, a guideline should be developed for the prompt recognition and management of CMV gastrointestinal lesions.
DISCLOSURESAuthor contributions: Z. Zaman and S. Lund reviewed the literature and drafted the manuscript. Z. Jalil and NK Seetlani edited the manuscript.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
REFERENCES 1. Beany A, Rainis T. CMV-related gastric ulcer and gastroduodenitis in an immunocompetent patient: A case report and literature review. Case Rep Gastrointest Med. 2021;2021:3513223. 2. Suter WR, Neuweiler J, Borovicka J, Binek J, Fantin AC, Meyenberger C. Cytomegalovirus-induced transient protein-losing hypertrophic gastropathy in an immunocompetent adult. Digestion. 2000;62(4):276–9. 3. Himoto T, Goda F, Okuyama H, et al. Cytomegalovirus-associated acute gastric mucosal lesion in an immunocompetent host. Intern Med. 2009;48(17):1521–4. 4. Crespo P, Dias N, Marques N, Saraiva da Cunha J. Gastritis as a manifestation of primary CMV infection in an immunocompetent host. BMJ Case Rep. 2015;2015:bcr2014206991. 5. Claeys M, Cool M, Lambrecht GL, Hertveldt K, Alliet G, Deboever G. CMV gastritis in the immunocompetent host. Acta Gastroenterol Belg. 2015;78(2):244–5. 6. Choi SW, Chung JP, Song YK, et al. Lower gastrointestinal bleeding due to cytomegalovirus ileal ulcers in an immunocompetent man. Yonsei Med J. 2001;42(1):147–51. 7. Monrobel A, Chicano M, Navarrese A, Martínez L, Zambrana JL. Gastrointestinal affectation with cytomegalovirus in an immunocompetent patient. Rev Esp Enferm Dig. 2006;98(11):881–2. [English, Spanish.] 8. Setakhr V, Muller G, Hoang P, Lambert AS, Geubel A. Cytomegalovirus-associated protein losing gastropathy in an immunocompetent adult: A case report. Acta Gastroenterol Belg. 2007;70(3):296–9.
Comments (0)