
Remember me





Metastasis of primary gastric cancer (GC) to the skin is quite rare. As a result, medical practitioners often misdiagnose or miss these malignant lesions altogether, leading to delays in treatment and worse outcomes. Incidence and mortality rates are highest in East Asia and a lower proportion of deaths occur in countries ranked higher in the United Nations' Human Development Index. However, there is still an overall predicted increase in the global incidence of GC from 1.1 million new cases and 770,000 deaths in 2020 to 1.8 million new cases and 1.3 million deaths in 2040.1 Therefore, practitioners will need to become more adept at recognizing and understanding the natural history of this rarer presentation of GC. Here, we review the case of a middle-aged man who presented for evaluation of a chronic rash involving the chest, neck, and face that was ultimately found to be metastatic adenocarcinoma with signet ring cell features (likely gastric vs gastroesophageal junction source) after skin biopsy.
CASE REPORTA 48-year-old man with a history of isolated left parotid gland enlargement presented to an outside institution with a skin rash involving his face, anterior neck, and upper chest wall. Several months prior, he had noticed a single, isolated, cutaneous lesion on his anterior neck that, over a few weeks, expanded inferiorly and superiorly to involve the upper chest wall and upper neck and face, respectively (Figure 1). He was initially prescribed oral antibiotics for a presumed skin and soft tissue infection. However, after treatment, his rash had worsened. By the time of presentation, the rash had developed palpable borders and was thick and leather-like in appearance. He also had experienced dysphagia, odynophagia, and 40 pounds of unintentional weight loss.
 Figure 1.:
Figure 1.: Cutaneous manifestation of metastatic adenocarcinoma from upper gastrointestinal source (likely gastric).
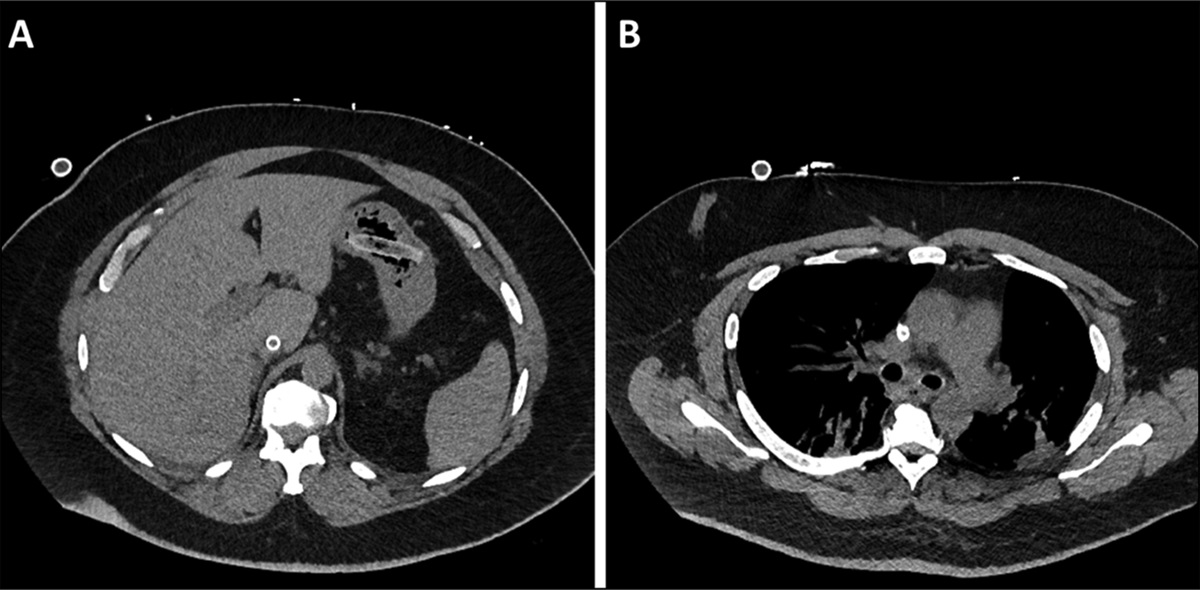
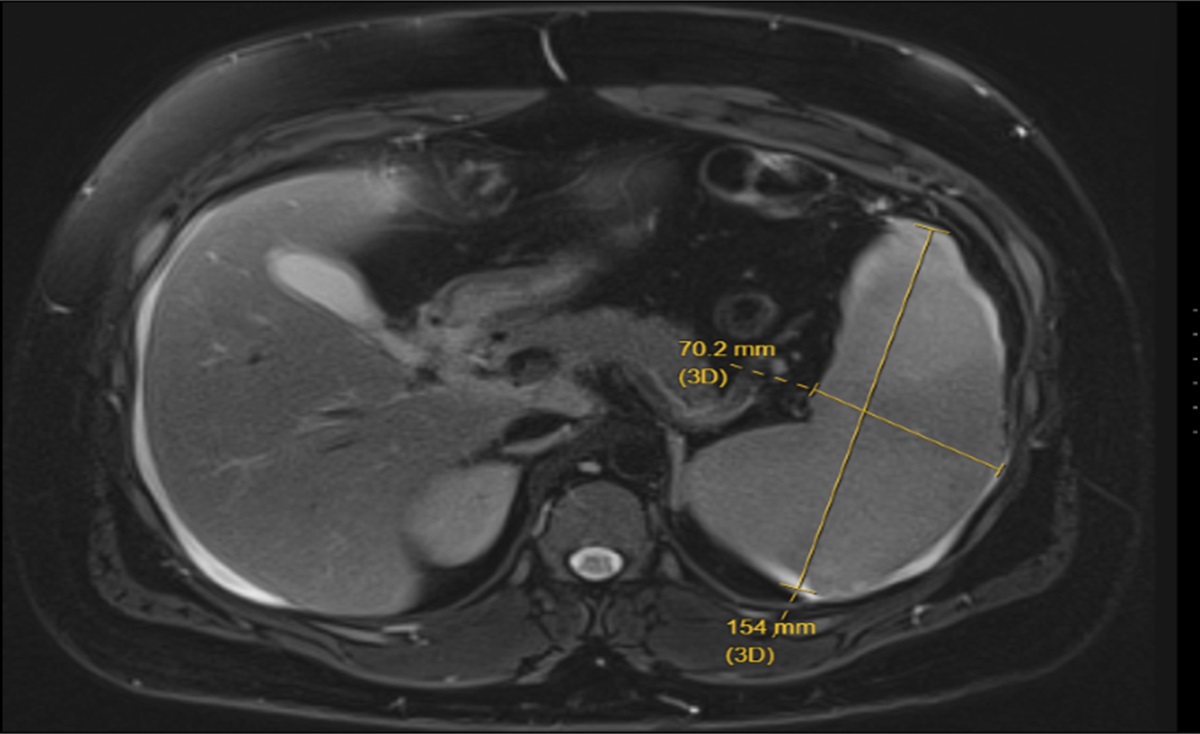
Initial diagnostic workup began at the outside facility and included a computed tomograph scan then magnetic resonance imaging of the affected area, which demonstrated anterior neck/chest wall skin thickening down to the subcutaneous fat, along with suspected sclerotic bony lesions throughout the visualized skeleton (concerning for metastasis). Given the radiological appearance of his skin, the initial differential included lymphoma vs an inflammatory process. The patient then underwent a punch biopsy of a right chest wall lesion. Immunostains of the skin biopsy were positive for CK7 and CDX2 but negative for p63, TTF1, CK5/6, CD45, S100, and SOX10. Combined with the morphologic features, this profile favored a poorly differentiated adenocarcinoma from luminal upper gastrointestinal origin.
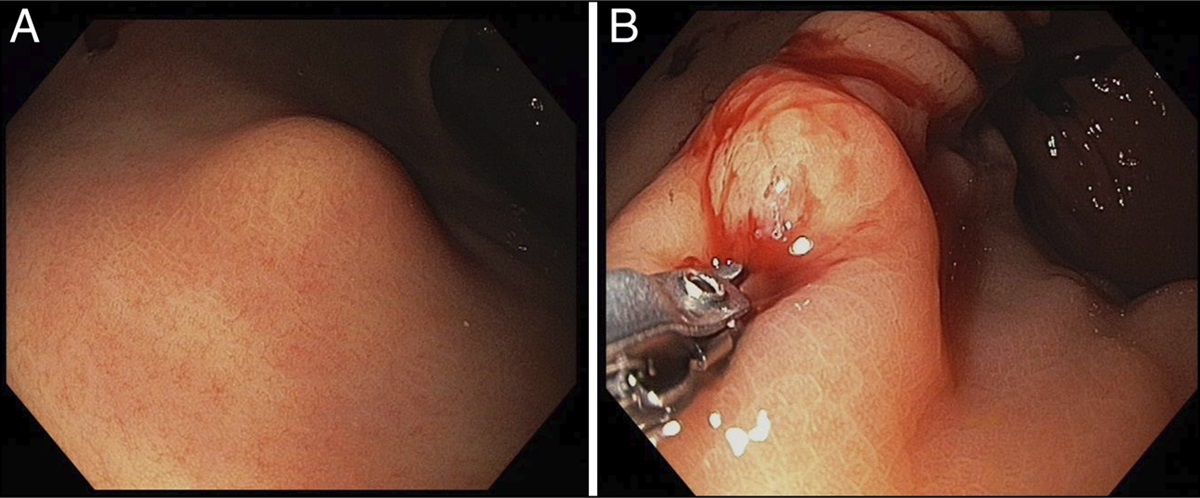
The patient subsequently presented to our institution for an esophagogastroduodenoscopy for further diagnostic workup. From the esophagogastroduodenoscopy, a large, noncircumferential submucosal mass on the greater curvature of the stomach was found, without evidence of prior or active bleeding; a second large infiltrative, fungating, circumferential mass, which was grossly suspected to represent a metastatic satellite lesion, was identified and involved the cardia, gastric fundus, and gastric body (Figure 2, greater curvature mass; Figure 3). Biopsies of the fungating mass and esophageal lesions were positive for poorly differentiated adenocarcinoma with signet ring cell features (Figures 4 and 5). To complete staging, a positron emission tomography/computed tomography demonstrated evidence of hypermetabolic activity involving the thoracic esophagus, gastric cardia, and greater curvature of the stomach; hypermetabolism in the anterior chest, neck, and head, in line with the area of the patient's rash; and several sclerotic lesions throughout the spine, pelvis, and ribs, consistent with bony metastases. Ultimately, he underwent chemotherapy treatment with repeat positron emission tomography/computed tomography imaging at the end of treatment showing decreased metabolic activity at the involved sites.
 Figure 2.:
Figure 2.: Noncircumferential submucosal mass of the greater curvature of the stomach as seen on upper endoscopy.
 Figure 3.:
Figure 3.: Fungating circumferential mass of the gastric body as seen on upper endoscopy.
 Figure 4.:
Figure 4.: 100× magnification, hematoxylin and eosin-stained biopsy of gastric mucosa.
 Figure 5.:
Figure 5.: 200× magnification, hematoxylin and eosin-stained biopsy of gastric mucosa. Arrowheads highlight the tumor cells infiltrating in the lamina propria of the gastric mucosa.
DISCUSSIONCutaneous metastasis of primary tumors remains very rare, with under 2% of all cutaneous lesions representing metastatic disease.2,3 It is most commonly seen with breast, lung, or colon primary tumors; regarding GC, 0.8% of cases may metastasize to the skin.4,5 Mechanisms of translocation of GC are still unclear, but proposed ideas include hematogenous/lymphatic spread, migration through remnant embryological ligaments, and direct tissue invasion of local microenvironments.6
Owing to the low number of reported cases in the medical literature, the natural progression of cutaneous GC is unknown. The most commonly affected body surface areas are the neck, back, and abdomen, although the face can be involved.7 Grossly, these lesions appear as singular or grouped nodules, often with erythematous bases. Less commonly, as in our case, lesions may resemble skin and soft tissue infections (eg, cellulitis and erysipelas), leading some patients to be inappropriately treated with antibiotics. Thus, cutaneous biopsies serve an integral role in determining the correct diagnosis.
Using the World Health Organization's GC classification system, our patient's cancer can be subclassified as a likely gastric adenocarcinoma with signet ring cell features, meaning less than 50% of the tumor is composed of mucin-producing signet ring cells. Signet ring cell involvement has been believed to influence several tumor characteristics, including cancer aggressiveness, metastatic organotropism, and prognosis.8 Similar to previously published cases of GC with signet ring cells, our patient had no metastatic involvement of the liver, lymph nodes, or peritoneum9 (the most common metastatic sites in GC). Despite first-pass physiology and apparent hematogenous spread of this patient's cancer (evidenced by cutaneous and osseous involvement), he did not have active disease in the liver. One potential reason for this is signet ring cell predilection towards bone and less commonly, skin.9 Unfortunately, 10-year survival in patients with signet ring cell GC remains poor (∼16%) with a median survival time of 10.2 months. By the time most patients are diagnosed with signet ring cell GC, over 75% have poor grade differentiation and 74.1% of cases have regional (31.1%) or distant (43%) site involvement.10 Prognostic data for signet ring cell cutaneous GC (CGC) are quite limited, although most patients with CGC of all cell types die within several months of diagnosis.5 Additional research into signet cell components for these cancer types is warranted as this could be an area of targeted treatment in the future.
Although rare, gastroenterologists should be cognizant of CGC in patients who present with cutaneous lesions in the setting of concerning gastrointestinal symptoms (eg, weight loss, dysphagia, odynophagia) as this may expedite potential endoscopic evaluation, diagnosis, and interventions.
DISCLOSURESAuthor contributions: A. Garcia: involved in the conception, acquisition, analysis, and interpretation of data for the manuscript; drafting and reviewing the manuscript; final approval of the version to be published; and agreeing to be accountable for all aspects of the manuscript in question. A. Maqsudlu: involved in the analysis and interpretation of data for the manuscript; drafting and reviewing the manuscript; final approval of the version to be published; and agreeing to be accountable for all aspects of the manuscript. I. Dhawan and A. Chaaya: involved in the conception, acquisition, analysis, and interpretation of data; reviewing the manuscript; final approval of the version to be published; and agreeing to be accountable for all aspects of the manuscript. A. Chaaya is the article guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
REFERENCES 1. Morgan E, Arnold M, Camargo MC, et al. The current and future incidence and mortality of gastric cancer in 185 countries, 2020–40: A population-based modelling study. EClinicalMedicine. 2022;47:101404. 2. Fernández-Antón Martínez MC, Parra-Blanco V, Avilés Izquierdo JA, Suárez Fernández RM.Cutaneous metastases of internal tumors. Actas Dermosifiliogr. 2013;104(10):841–53. 3. Betlloch-Mas I, Soriano-García T, Boira I, et al. Cutaneous metastases of solid tumors: Demographic, clinical, and survival characteristics. Cureus. 2021;13(11):e19970. 4. Namikawa T, Munekage E, Munekage M, et al. Subcutaneous metastasis arising from gastric cancer: A case report. Mol Clin Oncol. 2017;6(4):515–6. 5. Yang S, Liu XL, Guo XL, et al. Solitary metastasis to the skin and colon from gastric cancer after curative gastrectomy and chemotherapy: A case report. Medicine (Baltimore). 2020;99(31):e21532. 6. Narasimha A, Kumar H. Gastric adenocarcinoma deposits presenting as multiple cutaneous nodules: A case report with review of literature. Turk Patoloji Derg. 2012;28(1):83–6. 7. Şahin M, Ekinci F, Çelik C, Temiz P, Erdoğan AP, Göksel G. A rare case report of skin metastasis in gastric cancer. J Gastrointest Cancer. 2021;52(3):1156–8. 8. Marano L, Ambrosio MR, Resca L, et al. The percentage of signet ring cells Is inversely related to aggressive behavior and poor prognosis in mixed-type gastric cancer. Front Oncol. 2022;12:897218. 9. Bajoghli AA, Piselli A, Kemprecos H, Khosravi H, Cardis MA, Noel MS. Gastric carcinoma's primary presentation as multiple cutaneous nodules throughout the body. Cancer Treat Res Commun. 2022;31:100532. 10. Benesch MGK, Mathieson A. Epidemiology of signet ring cell adenocarcinomas. Cancers (Basel). 2020;12(6):1544.
Comments (0)