
Remember me





Pancreatic TB is caused by mycobacterium tuberculosis (MTB) that commonly affects immunocompromised individuals. Although TB is prevalent worldwide, pancreatic TB remains exceedingly rare, with a reported incidence of less than 4.7% in a 1944 autopsy series of patients with TB and 2% in a similar study in 1966.1 The incidence, however, has been on the rise for the past few decades, possibly due to improvement in imaging techniques and the increase in the number of immunocompromised individuals in the community, such as those with HIV or patients receiving immunosuppressive therapy.2 In addition, there are conditions such as pancreatic neoplasms that can present similarly to pancreatic TB, potentially leading to unnecessary surgical interventions, which carry their own risks. Therefore, in patients positive for MTB or with risk factors of TB, pancreatic lesions should prompt early use of endoscopic ultrasound (EUS) with fine-needle aspiration. This approach can confirm the diagnosis of a treatable condition and avoid unnecessary invasive procedures for diagnosing other conditions with similar presentations.
CASE REPORTA 38-year-old man from Honduras presented with 3 days of epigastric pain and large-volume hematochezia. He also reported fever, night sweats, and abdominal pain for 2 months. Vital signs showed blood pressure of 86/52 mm Hg, heart rate of 119 beats/min, and temperature of 102.7°F. Oral thrush and cachexia were noted on physical examination. Laboratory test results revealed hemoglobin of 5.3 g/dL and positive HIV with a CD4 count of 11 cells/μL. Hypotension responded to fluids, and the patient received 3 units of blood after which his hemoglobin increased from 5.3 to 9 g/dL. Given suspicious immigration history and HIV-AIDS with the background of chronic, intermittent fevers and night sweats, extrapulmonary tuberculosis was high on differentials prompting investigation. Acid fast bacillus (AFB) blood culture returned positive for MTB DNA after which antitubercular treatment (ATT) was started for disseminated TB. To better understand his abdominal symptoms, abdominal computed tomography with intravenous contrast was pursued, which showed multiple peripancreatic fluid collections with dependent air, suspicious of fistula with adjacent bowel (Figure 1). Four days later, he had 4 bloody bowel movements, dropping his hemoglobin to 5.8 and blood pressure to 93/67. Urgent abdominal computed tomography did not reveal any active gastrointestinal bleeding, and our patient underwent upper endoscopy and colonoscopy the next day after this event. Upper endoscopy revealed a duodenal ulcer and suspected fistula in the anterior duodenal sweep (Figure 2). Colonoscopy was largely normal. After a month of stability on ATT, the patient spiked a new fever. EUS was pursued as a workup for the new fever. Pancreatic collections were aspirated and grew acid fast bacilli consistent with TB (Figure 3). In the interim, the duodenal ulcer with suspected fistula had completely healed and pancreatic collections had reduced in size on repeat imaging (Figure 4). Interestingly, the patient had completed more than 1 month of ATT by that time. As for the cause of duodenal ulcer, biopsies were negative for AFB, Helicobacter pylori, cytomegalovirus, leishmaniasis, and human herpes virus-8. There was no history of non-steroidal anti inflammatory drug (NSAID) use, but our patient had been smoking cigarettes for 26 years.
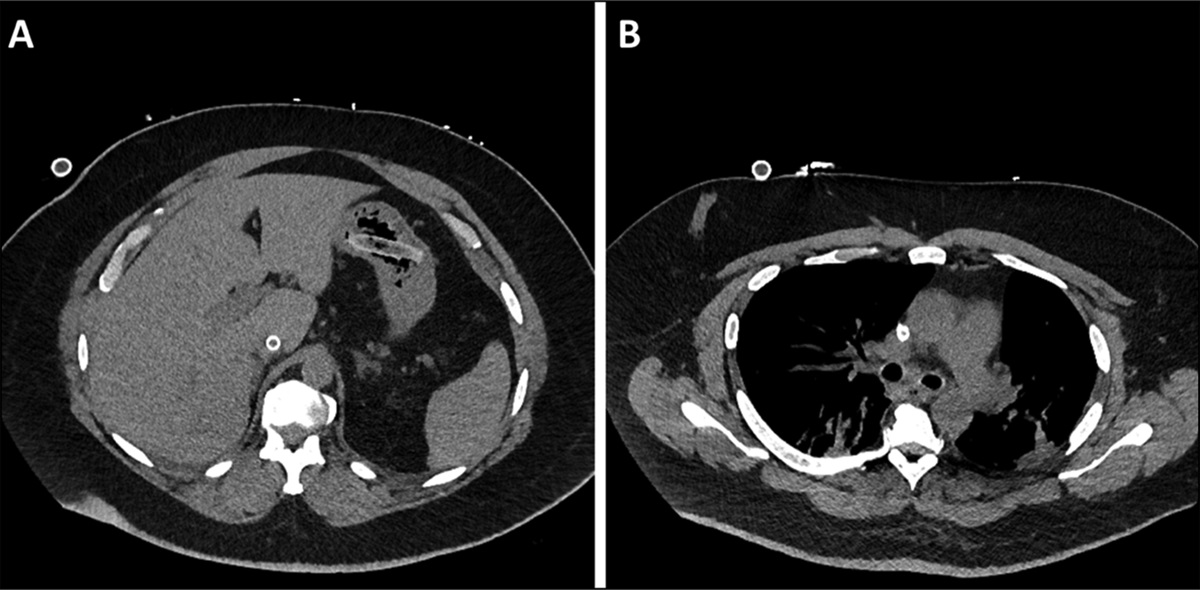
 Figure 1.:
Figure 1.: (A) Complex peripancreatic fluid collections largest 5.4 cm at the proximal body of the pancreas. (B) 4.8 cm complex peripancreatic fluid collection at the distal body and tail of the pancreas. (C) Dependent gas seen in peripancreatic fluid collection, suspicious for a fistula with adjacent bowel.
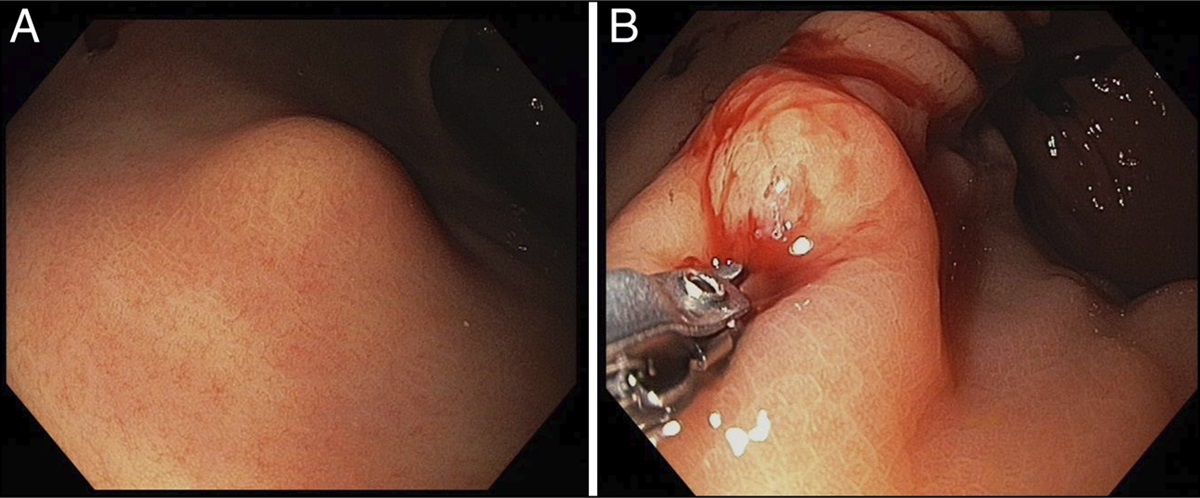
 Figure 2.:
Figure 2.: Upper endoscopy image showing a duodenal ulcer and a fistulous opening (yellow arrow) in the anterior duodenal sweep.
 Figure 3.:
Figure 3.: Microscopic view of acid fast bacilli grown from aspirated pancreatic collections. (600x).
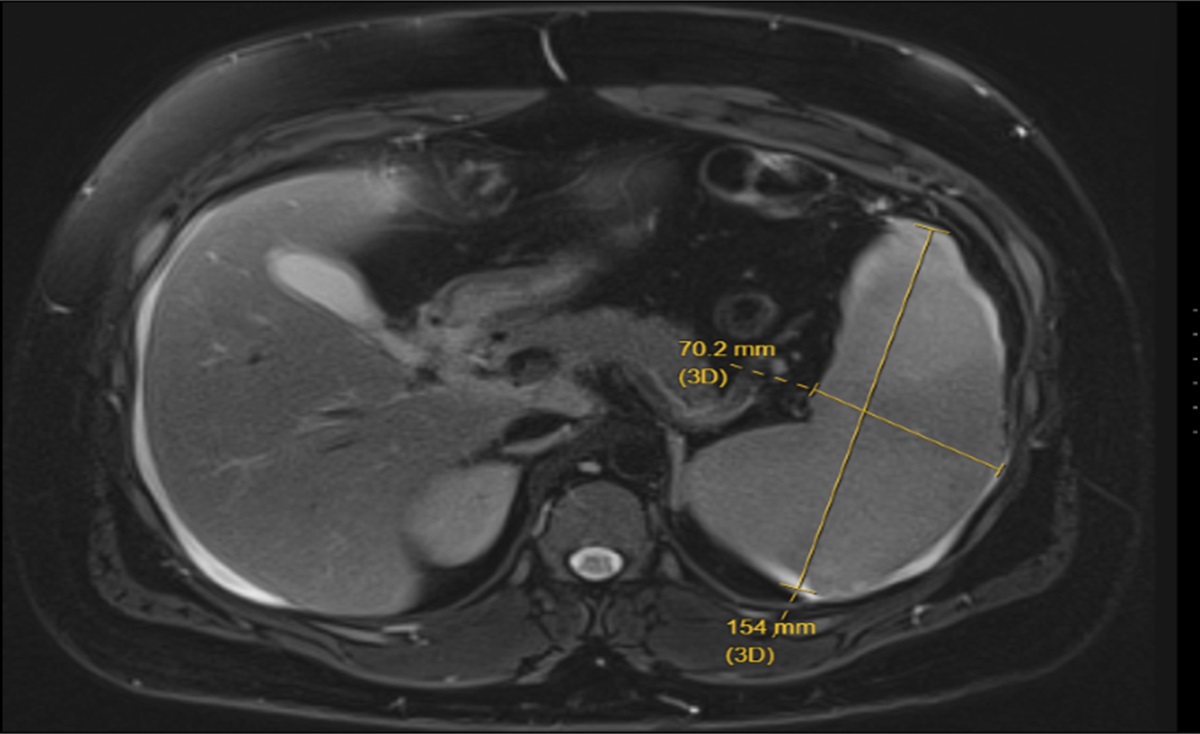
 Figure 4.:
Figure 4.: EUS image showing aspiration needle (white line) in pancreas head cyst.
DISCUSSIONThe abdominal cavity is a common site for extrapulmonary tuberculosis, yet pancreatic involvement remains rare, even in endemic areas of TB. This rarity is likely due to the protective effect of pancreatic enzymes against MTB.3,4 The routes of MTB spread to the pancreas include hematogenous spread, ingestion of sputum containing the organism, and direct spread from adjacent organs.5 The most common location of involvement in the pancreas is the head, followed by the body, uncinate process, and then the tail.6
Pancreatic TB can present in a variety of ways including abdominal pain with fever and weight loss, upper GI bleeding (UGIB), obstructive jaundice, pancreaticobiliary fistula, acute or chronic pancreatitis, and portal hypertension. Debnath et al reported a patient who presented with abdominal pain and was found to have pancreatic TB with a fistula to the duodenum.6 Panic et al conducted a comprehensive systematic review and identified 116 studies describing pancreatic TB in 166 patients between 1978 and 2017.2 The most common symptoms in these patients were abdominal pain, followed by weight loss and fever. Our patient presented with acute UGIB and had been suffering from chronic abdominal pain, fever, and weight loss for 2 months. Pancreatic TB presenting with UGIB is rare, with few cases reported in the literature. Fan et al reported a case in 1984 diagnosed postmortem after massive GI bleeding.7 Cheng et al described a patient with massive UGIB that had necessitated transarterial embolization after efforts to control the bleeding by endoscopy and the surgery failed.8 Irfan et al mentioned how the source of UGIB in patients with pancreatic TB can be due to splenic artery pseudoaneurysm.9 In our case, UGIB was likely due to a duodenal ulcer or a fistulous tract between the pancreas and the GI tract. Despite initial AFB-negative biopsy results of the ulcer, both conditions were likely related to TB, as indicated by complete resolution after a month of ATT and no other significant risk factors.
The most important risk factor of pancreatic TB among 116 patients studied by Panic et al was HIV-positive status (22%). Our patient was HIV-positive with a severely low CD4 count of 11; in addition, he was from a TB-endemic country. Pancreatic TB often poses a diagnostic dilemma. A clue to diagnosis is the presence of active extra-abdominal TB, which should raise suspicion of a tubercular etiology in a patient with abdominal complaints. Workup includes abdominal imaging, such as computed tomography and magnetic resonance imaging, and direct histopathological examination, preferably by EUS or ultrasound/computed tomography-guided biopsy. Laparotomy, given its invasiveness, should be a last resort.
Treatment of upper gastrointestinal bleeding in patients with pancreatic TB can be challenging due to the acute massive presentation in some cases and the underlying tissue fragility and necrosis caused by the tuberculous infection. A multidisciplinary approach, including endoscopic, surgical, and interventional radiologic techniques, may be required.8 Management of pancreatic TB and its local complications, such as fistula tracts, is similar to that of pulmonary TB, with standard antituberculous therapy. Most patients have good and complete response to therapy.1 A few studies described performing a Whipple procedure for a suspicious pancreatic mass that was eventually diagnosed as pancreatic TB.10,11 Therefore, pancreatic lesions in a patient positive for MTB or with risk factors of TB should warrant an early EUS with fine-needle aspiration. This approach can confirm the diagnosis of a treatable condition; prevent unnecessary invasive procedures for diagnosing conditions with similar presentations, such as pancreatic cancer; and help avoid surgical management of bowel fistulas.
DISCLOSURESAuthor contributions: D. Zaffar was involved in clinical care of this patient. D. Zaffar also wrote the manuscript and reviewed the literature. CB Ranabhat, A. Ismail, G. Gonga, and S. Hossain also contributed to the manuscript writing. GV Rodriguez, D. Sharma, and K. Raymond reviewed and edited the manuscript. R. Kim is the article guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this manuscript.
REFERENCES 1. Chaudhary P, Bhadana U, Arora MP. Pancreatic tuberculosis. Indian J Surg. 2015;77(6):517–24. 2. Panic N, Maetzel H, Bulajic M, Radovanovic M, Löhr JM. Pancreatic tuberculosis: A systematic review of symptoms, diagnosis and treatment. United Eur Gastroenterol J. 2020;8(4):396–402. 3. Sharma SK, Mohan A. Extrapulmonary tuberculosis. Indian J Med Res. 2004;120(4):316–53. 4. Ali M, Shaukat A, Al-Suwaidi Z, Al-Maslamani M. Tuberculosis of pancreas, the first case reported from Qatar. Int J Mycobacteriol. 2019;8(1):101–3. 5. Debi U, Ravisankar V, Prasad KK, Sinha SK, Sharma AK. Abdominal tuberculosis of the gastrointestinal tract: Revisited. World J Gastroenterol. 2014;20(40):14831–40. 6. Debnath P, Jain S, Junare P, et al. Primary pancreatic tuberculosis with a duodenal fistula in an immunocompetent young man. Clin J Gastroenterol. 2021;14(5):1567–70. 7. Fan ST, Yan KW, Lau WY, Wong KK. Tuberculosis of the pancreas: A rare cause of massive gastrointestinal bleeding. Br J Surg. 1986;73(5):373. 8. Cheng CW, Tsou YK, Fan GW, et al. Duodenal bleeding caused by pancreatic tuberculosis in a patient with AIDS and disseminated tuberculosis. Endoscopy. 2012;44(Suppl 2 UCTN):E34–5. 9. Irfan M, Thiavalappil F, Nagaraj J, et al. Tuberculous pancreatitis complicated by ruptured splenic artery pseudoaneurysm. Monaldi Arch Chest Dis. 2013;79(3-4):134–5. 10. Liu H, Zhu J, Dong H, et al. Isolated hepatic tuberculosis in the caudate lobe mimicking intrahepatic carcinoma. Clin Res Hepatol Gastroenterol. 2017;41(5):e65–7. 11. Saluja SS, Ray S, Pal S, et al. Hepatobiliary and pancreatic tuberculosis: A two decade experience. BMC Surg. 2007;7:10.
Comments (0)