
Remember me





Hepatic artery aneurysms (HAAs) make up approximately 14%–20% of visceral artery aneurysms. Most HAAs do not display any symptoms. While uncommon, instances of obstructive jaundice have been documented as a result of external compression on the bile duct, or the rupture of the HAA into the biliary system may lead to obstructive jaundice secondary to hemobilia.1
CASE REPORTA 85-year-old woman with a history of embolic atrial fibrillation on anticoagulation, hyperthyroidism treated with amiodarone, and atheromatous stenosis of the internal carotid arteries estimated at 40%. She had been suffering from continuous cholestatic mucocutaneous jaundice without remission for a week, without fever or abdominal pain. The physical examination revealed jaundice in an afebrile patient with a normal heart rate and blood pressure and a body mass index of 28 kg/m2.
Biochemically, her total bilirubin levels were elevated at 133 μmol/L (normal range [NR] < 17 μmol/L); conjugated bilirubin 93 μmol/L (NR < 10 μmol/L); alkaline phosphatase 577 U/L (NR: < 150 UI/L); gamma-glutamyl transferase 1,370 U/L (NR < 35 UI/L); aspartate transaminase 141 UI/L (NR < 45 UI/L); alanine transaminase 183 UI/L (NR < 55UI/L); and prothrombin level at 71%, with no biological signs of inflammation or organ failure.
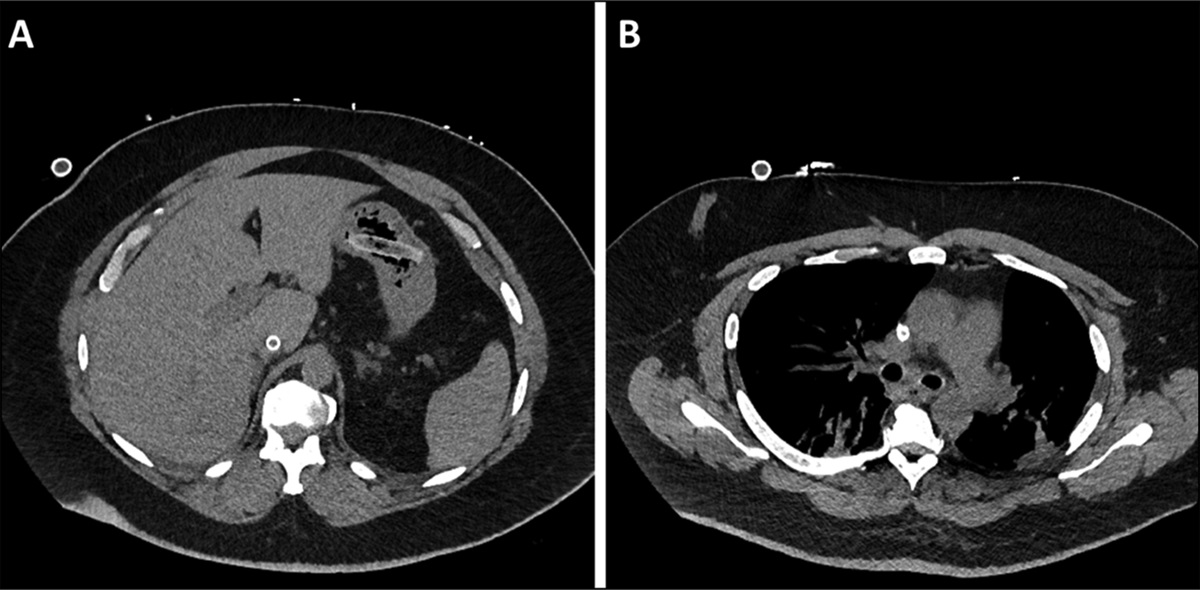
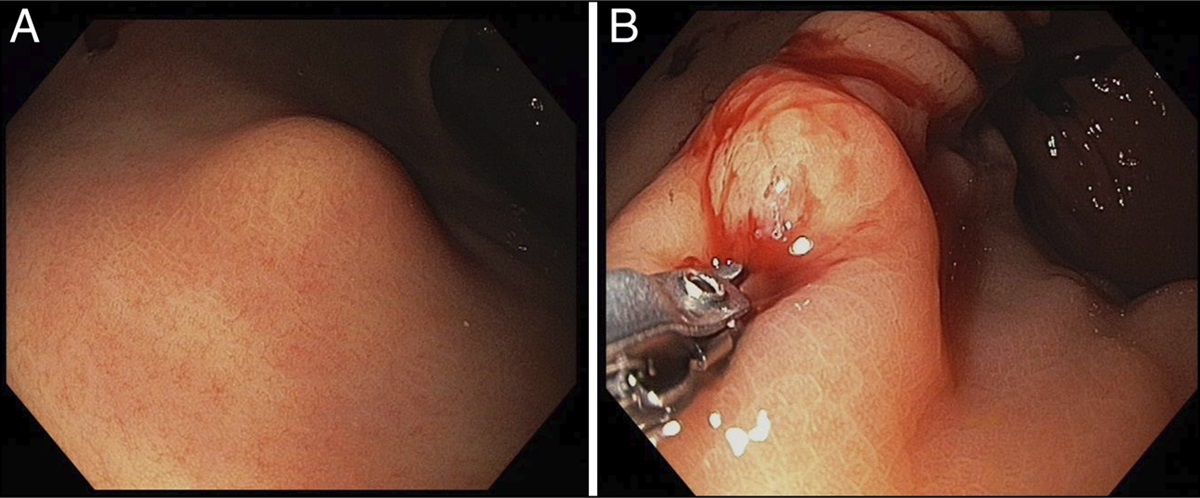
An abdominal ultrasound (US) showed dilatation of the intrahepatic bile ducts and the main bile duct with no visible obstruction. A computed tomography (CT) scan showed homogeneous, hypervascular lesion with well-defined borders, with more intense enhancement during the portal and late phases measuring 23 × 37 mm (Figure 1). Endoscopic US showed an anechoic lesion with turbular flow on color Doppler, completed with contrast enhancement (Figure 2), compressing the common bile duct suggestive of a probable HAA (Figure 3).
 Figure 1.:
Figure 1.: Coronal reconstruction of an enhanced CT scan revealing a compressive hepatic artery aneurysm (red arrow) leading to the dilation of the main bile duct SMA (blue arrow). CT, computed tomography
 Figure 2.:
Figure 2.: Transbulbar contrast-enhanced endoscopic ultrasound image showing a hepatic artery aneurysm before (A) and after (B) contrast injection. HAA, hepatic artery aneurysm.
 Figure 3.:
Figure 3.: Transbulbar station echoendoscopy showing a hepatic artery aneurysm responsible for dilation of the common bile duct. HAA, hepatic artery aneurysm.
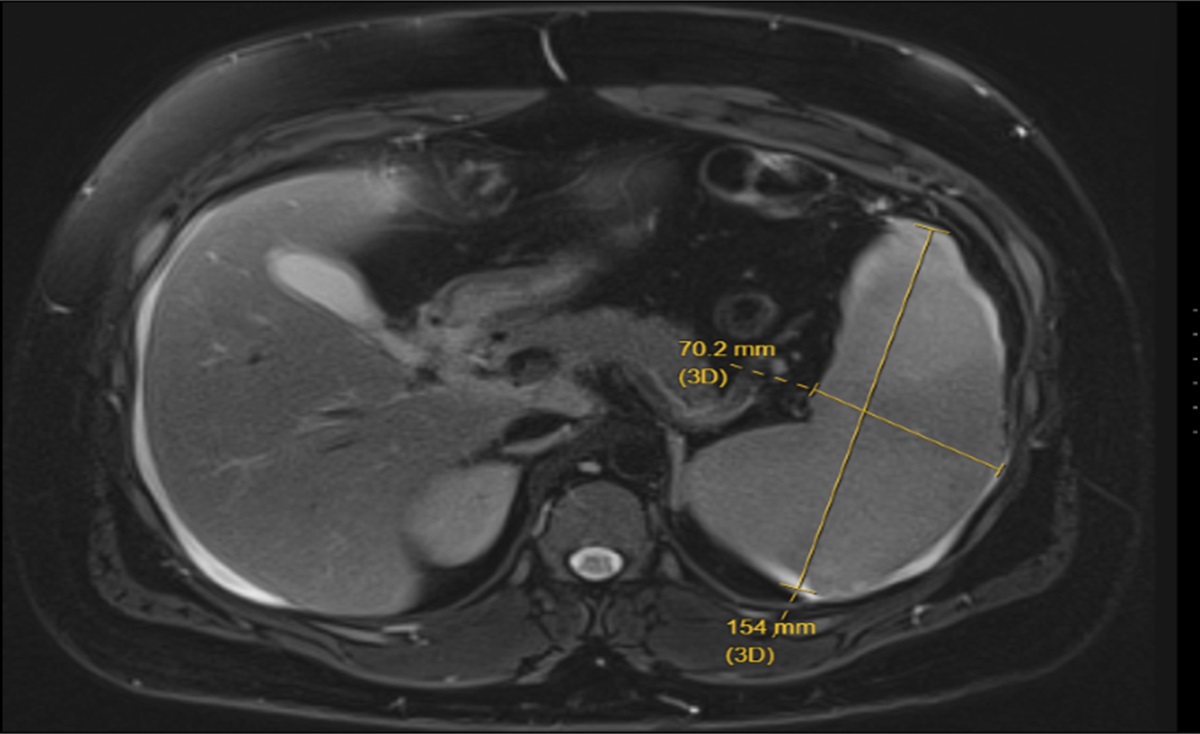
The therapeutic management was based on radiological embolization of the hepatic artery, which was performed without complications. Follow-up CT scans showed persistent dilatation of the bile ducts upstream of a thrombosed aneurysm (Figure 4). A week later, biliary calibration was performed by endoscopic retrograde cholangiopancreatography with the placement of a 6 cm fully covered metallic stent.
 Figure 4.:
Figure 4.: Coronal reconstruction of an enhanced CT scan after the embolization of the hepatic artery aneurysm (red arrow). CT, computed tomography.
Follow-up, 8 weeks later, showed the disappearance of jaundice with normalization of liver tests (aspartate transaminase: 40 UI/L, alanine transaminase: 44 UI/L, bilirubin: 14 μmol/L, alkaline phosphatase: 123 UI/L, gamma-glutamyl transferase: 39 UI/L), and the biliary stent was removed after 6 months of calibration. After consultation with internists and vascular surgeons, no further etiological workup was conducted, given the patient's age.
DISCUSSIONWithin the category of visceral aneurysms, HAAs are considered relatively rare, accounting for approximately 14%–20% of all visceral artery aneurysms. They rank as the second most prevalent location for aneurysms in the splanchnic circulation, trailing only behind the splenic artery. The overwhelming majority of HAAs are solitary in nature and are located extrahepatically. The pathophysiology remain not entirely elucidated.1 Typically, their etiology is attributed to atherosclerosis, trauma, or iatrogenic factors. These aneurysms tend to be more frequent in men, in a ratio of 2:1, and predominantly manifest during the sixth decade of life.1 The precise incidence remains uncertain, a retrospective study conducted at the Mayo Clinic estimating the incidence to be approximately 0.002%.3
Most of the HAAs are asymptomatic, and 60%–80% of the patients are diagnosed when the aneurysm has complicated with bleeding or rupture, or, as in our case, with obstructive jaundice due to external bile duct compression.2 Moreover, jaundice may also result from the rupture of the HAA into the biliary system may lead to obstruction of the main bile duct secondary to hemobilia, which represents clinically by Quinke triad (abdominal pain, gastrointestinal bleeding, and jaundice). In addition, HAA may present in atypical forms such as cholangitis and portal hypertension.4 Irrespective of clinical presentation, the diagnosis of HAA is always based on imaging including US, CT scan, CT angiography, magnetic resonance imaging, endoscopic ultrasonography, and angiography. Angiography is considered a preferred therapeutic approach for splanchnic aneurysms, often involving embolization. It is worth noting that multidetector computed tomographic angiography has demonstrated excellent diagnostic accuracy for HAAs, with a reported sensitivity and specificity of 100%.5
Various treatment options exist for HAAs ranging from observation to surgical resection. Various surgeries including hepatic resection for large intrahepatic aneurysm, excision and use of arterial or venous jump graft, bypass with jump graft, and ligation. The decision on the surgical strategy for repair depends on location, size, and feasibility of interventional radiology approaches. If collateral circulation is not sufficient, the aneurysmal artery needs to be reconstructed or partial hepatectomy might be required. Intrahepatic aneurysm, on the other hand, might be treated with endovascular techniques, either by stenting or embolization.6
For the treatment of benign biliary strictures, temporary insertion of multiple plastic stents, the maximum number of stents possible, every 3–4 months for a total duration of 12 months or of a fully covered metallic stent for 6 months is recommended.7
HAAs are rare, with only a few published cases. To our knowledge, this case appears to be the first reported in the literature where contrast-enhanced endoscopy was the diagnostic method. HAAs can give rise to complications (compression and rupture), hence the importance of appropriate radiological or surgical treatment.
DISCLOSURESAuthor contributions: W. El Ouardi is the article guarantor. Fatima Zahrae El Mansoury Conception and design of the work, Drafting the work, Final approval of the version to be published.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
REFERENCES 1. Rosenberg A, Trebska-McGowan K, Reichman T, et al. Management of hepatic artery aneurysm: A case series. Ann Hepatobiliary Pancreat Surg. 2020;24(3):333–8. 2. Julianov A, Georgiev Y.Hepatic artery aneurysm causing obstructive jaundice. Quant Imaging Med Surg. 2014;4(4):294–5. 3. Abbas MA, Fowl RJ, Stone WM, et al. Hepatic artery aneurysm: Factors that predict complications. J Vasc Surg. 2003;38(1):41–5. 4. Noor MT, Dutta U, Appasani S, Kochhar R, Singh K. Hepatic artery aneurysm: A rare presentation as cholangitis and portal hypertension. Gastrointest Endosc. 2012;75(1):190–1. 5. Haghighatkhah H, Sanei Taheri M, Kharazi SM, Zamini M, Rabani Khorasgani S, Jahangiri Zarkani Z. Hepatic artery aneurysms as a rare but important cause of abdominal pain; a case series. Arch Acad Emerg Med. 2019;7(1):e25. 6. Jana M, Gamanagatti S, Mukund A, et al. Endovascular management in abdominal visceral arterial aneurysms: A pictorial essay. World J Radiol. 2011;3(7):182–7. 7. Dumonceau J, Tringali A, Papanikolaou IS, et al. Endoscopic biliary stenting. Tando. 2016;30(1):43–50.
Comments (0)