
Remember me





Chronic octreotide is a risk factor for the development of gallstones (GS).1 For those who are symptomatic or have GS-related sequelae, cholecystectomy has become the gold standard.1–3 Percutaneous and endoscopic management have been used in patients who are poor surgical candidates, usually to treat acute complications such as cholecystitis.2,4,5 We present a case of endoscopic ultrasound (EUS)-guided cholecystoduodenostomy (EUS-CD) to extract GS in a patient with biliary colic and recurrent cholangitis in the setting of chronic octreotide-associated GS disease, where gallbladder (GB) decompression alone would not be sufficient to alleviate his symptoms or risk of cholangitis.
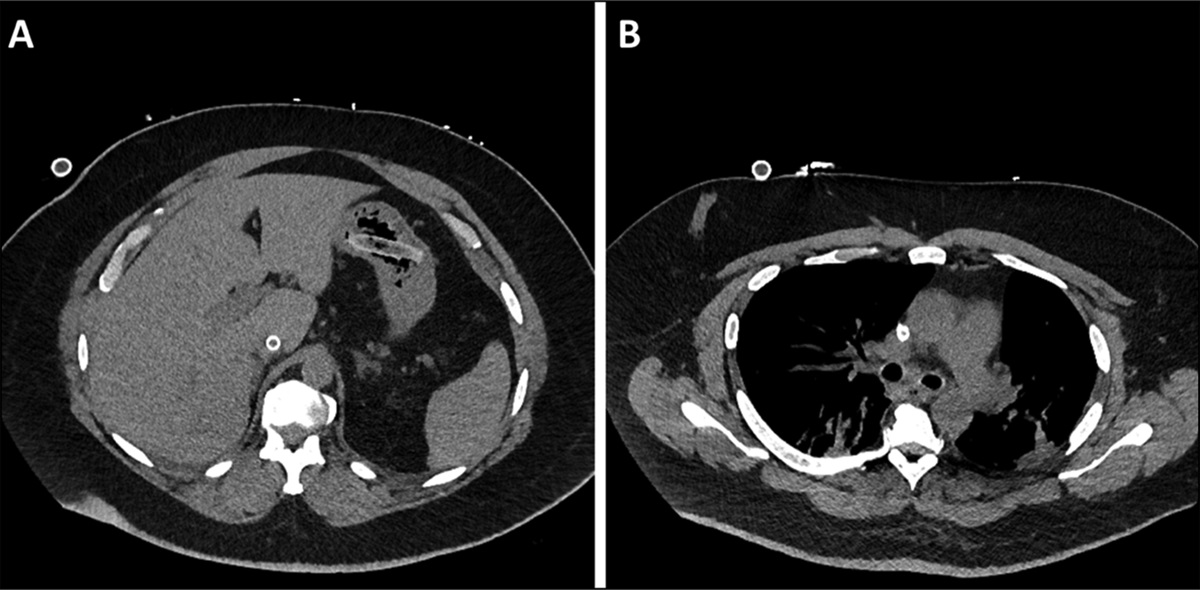
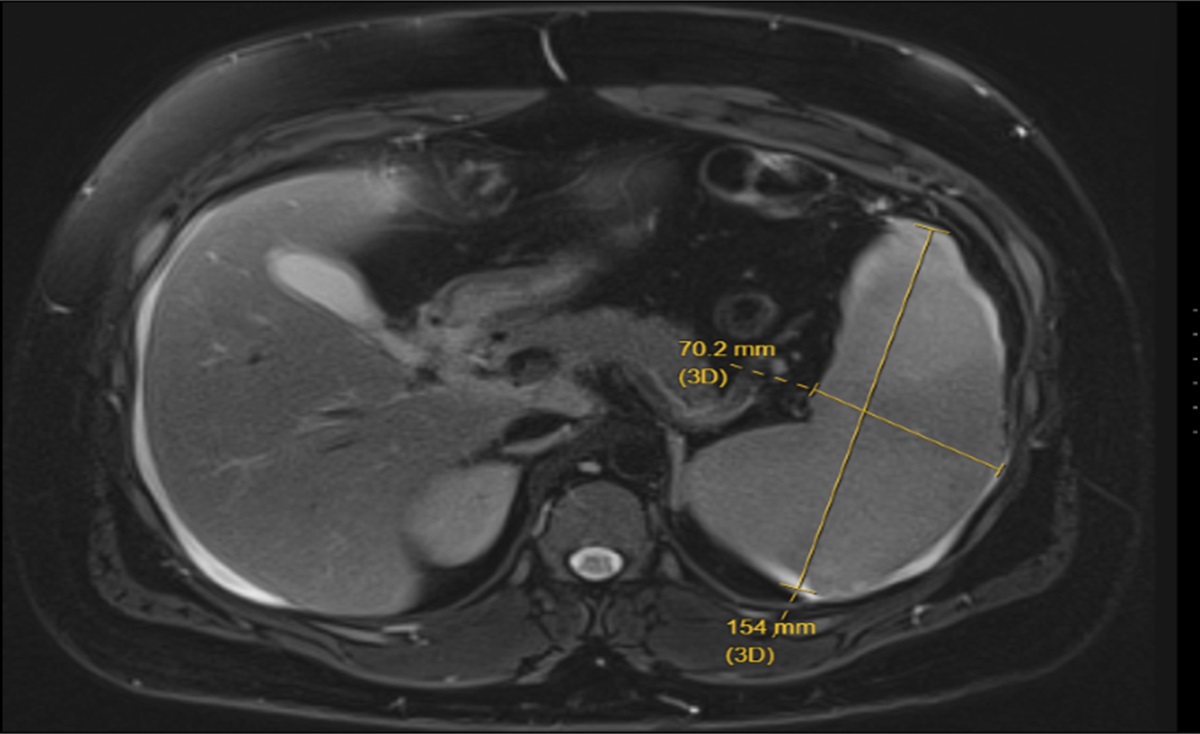
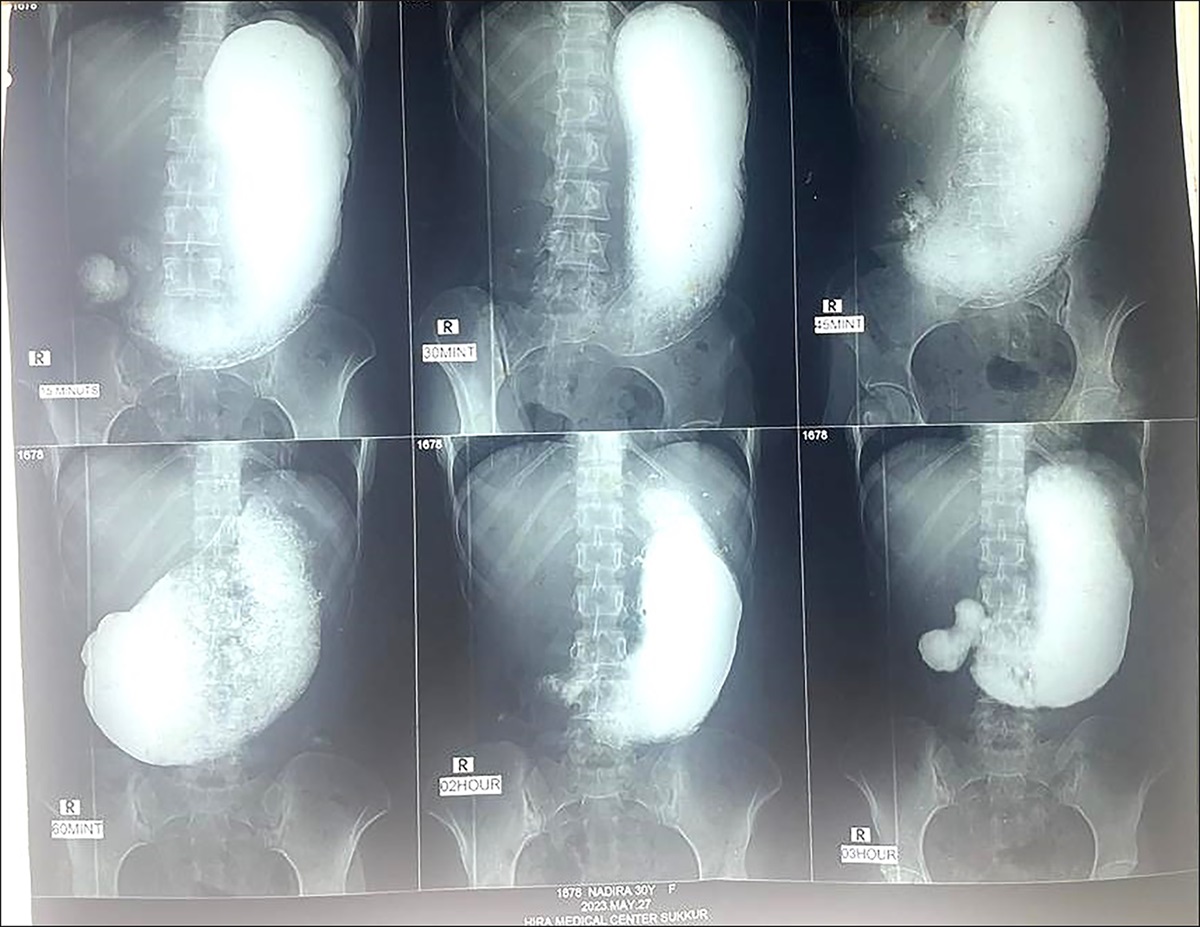
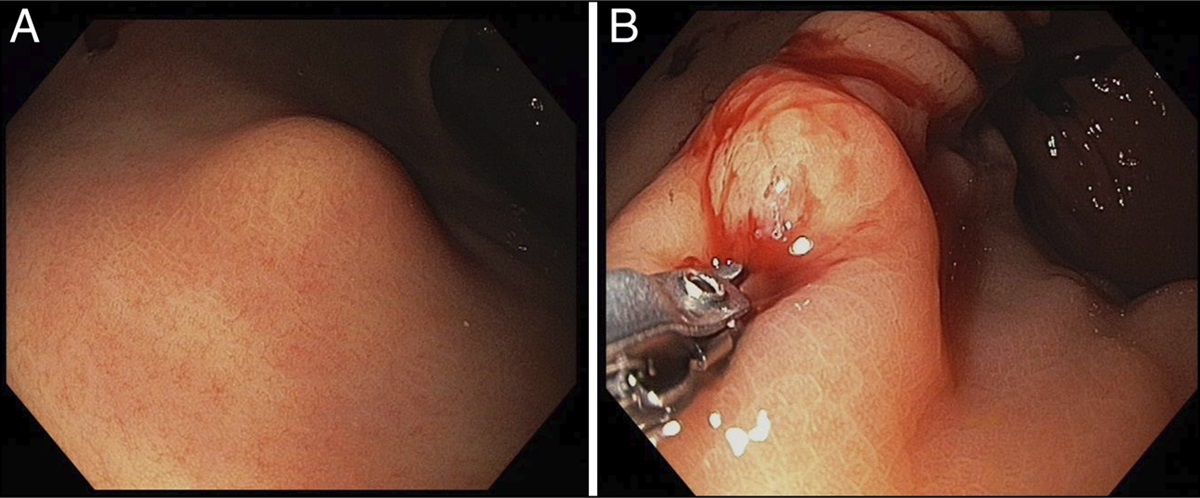
CASE REPORTA 74-year-old man with a history of metastatic pancreatic neuroendocrine tumor treated with distal pancreatectomy, left hepatectomy, transverse colectomy with colostomy, radiation therapy, and extended suppressive octreotide use was found to have innumerable GS after presenting with cholangitis and being treated with endoscopic retrograde cholangiopancreatography (ERCP) and sphincterotomy. He was on octreotide-LAR 60 mg every 3 weeks for 17 years before his first presentation of symptomatic GS disease. There was no evidence of GS going back to his imaging from before octreotide initiation. He was deemed a poor surgical candidate because of his numerous abdominal surgeries, radiation, and transverse colostomy overlying the right upper quadrant, which would need to be reversed for surgical cholecystectomy. His neuroendocrine tumor was stable and has not progressed in years. We opted to proceed with EUS-CD with stone extraction to reduce his risk of cholangitis and to alleviate his symptoms of biliary colic. Assessment with magnetic resonance cholangiopancreatography (MRCP) showed greater than 200 GS impacted in the GB (Figure 1). EUS-CD was performed free hand, with placement of a 10 × 10-mm lumen-apposing metal stent (LAMS). After allowing the tract to mature over 4 weeks and upsizing to a 15 × 10-mm LAMS, over 200 GS averaging 8–10 mm in size were extracted (Figures 2, 3) over 3 sessions by electrohydraulic lithotripsy, basket, and balloon sweep, resulting in complete removal of all GS from the GB, confirmed under fluoroscopy with contrast, and then MRCP (Figure 4). The cholecystoduodenal fistula patency was maintained long term with a double pigtail stent. Ursodiol was added to reduce the recurrence of GS because of his ongoing octreotide use. Six months later, he continues to do well without recurrence of cholangitis, biliary colic, nor evidence of GS disease on imaging.
 Figure 1.:
Figure 1.: MRCP with innumerable gallstones.
 Figure 2.:
Figure 2.: Extracting gallstones.
 Figure 3.:
Figure 3.: Extracting gallstones.
 Figure 4.:
Figure 4.: MRCP after complete extraction of gallstones.
DISCUSSIONOctreotide use is associated with GS formation; however, patients are usually asymptomatic and do not require surgical or medical therapy.2 In rare cases of chronic octreotide use, GS burden can be high and lead to biliary colic, cholangitis, and cholecystitis.2–4 The mechanism of octreotide-associated GS formation is believed to be attributed to GB stasis and modification of bile composition.1 This can lead to increased precipitation of cholesterol and calcium bilirubinate and subsequent stone formation.1
For those who are poor surgical candidates after initial decompression, EUS-CD offers an option for stone extraction. EUS-guided GB decompression was first described in 2007 for a poor surgical candidate with hilar cholangiocarcinoma and acute cholecystitis in which double pigtail biliary stents were used to drain the GB.6 Since the first description of the LAMS in 2012 and its use in GB drainage in 2015, the LAMS has become the most commonly used stent for this purpose.4,7,8
Although EUS-guided GB drainage with LAMS is reported frequently in literature for acute cholecystitis, this procedure's use in medication-induced GS disease is unique.4,9–11 We opted for this technique over others, such as transpapillary GB stenting, to completely extract our patient's GS because of his recurrent biliary colic and because of his significant stone burden as seen on the initial MRCP. There are no documented cases regarding EUS-CD for stone extraction for octreotide-associated GS burden. Our case highlights the successful option and expanding scope for endoscopic GS management.
DISCLOSURESAuthor contributions: All authors contributed evenly, including conception, data collecting/analysis, drafting/writing, and editing. S. Gupta is the article guarantor.
Financial disclosure: None to report.
Previous presentation: American College of Gastroenterology 2023 Meeting; October 23, 2023; Vancouver, British Columbia, Canada.
Informed consent was obtained for this case report.
REFERENCES 1. Ahrendt SA, McGuire GE, Pitt HA, Lillemoe KD. Why does somatostatin cause gallstones? Am J Surg. 1991;161(1):177–83. 2. Redfern JS, Fortuner WJ. Octreotide-associated biliary tract dysfunction and gallstone formation: Pathophysiology and management. Am J Gastroenterol. 1995;90(7):1042–52. 3. Ge N, Sun S, Sun S, Wang S, Liu X, Wang G. Endoscopic ultrasound-assisted transmural cholecystoduodenostomy or cholecystogastrostomy as a bridge for per-oral cholecystoscopy therapy using double-flanged fully covered metal stent. BMC Gastroenterol. 2016;16:9. 4. James T, Baron T. EUS-guided gallbladder drainage: A review of current practices and procedures. Endosc Ultrasound. 2019;8(Suppl 1):28–S34. 5. Cianci P, Restini E. Management of cholelithiasis with choledocholithiasis: Endoscopic and surgical approaches. World J Gastroenterol. 2021;27(28):4536–54. 6. Baron TH, Topazian MD. Endoscopic transduodenal drainage of the gallbladder: Implications for endoluminal treatment of gallbladder disease. Gastrointest Endosc. 2007;65(4):735–7. 7. Binmoeller KF, Shah JN. Endoscopic ultrasound-guided gastroenterostomy using novel tools designed for transluminal therapy: A porcine study. Endoscopy. 2012;44(5):499–503. 8. Irani S, Baron TH, Grimm IS, Khashab MA. EUS-guided gallbladder drainage with a lumen-apposing metal stent (with video). Gastrointest Endosc. 2015;82(6):1110–5. 9. Torres Yuste R, Garcia-Alonso FJ, Sanchez-Ocana R, et al. Safety and efficacy of endoscopic ultrasound-guided gallbladder drainage combined with endoscopic retrograde cholangiopancreatography in the same session. Dig Endosc. 2020;32(4):608–15. 10. Yuste RT, García-Alonso FJ, Sánchez-Ocana R, et al. Safety and clinical outcomes of endoscopic ultrasound-guided gallbladder drainage with lumen-apposing metal stents in patients with dwell time over one year. Ann Gastroenterol. 2019;32(5):514–21. 11. Wang W, Shi X, Jin Z, Li Z. Endoscopic laser lithotripsy and lithotomy through the lumen-apposing metal stent for a giant gallstone after EUS gallbladder drainage. VideoGIE. 2017;2(5):112–5.
Comments (0)