Type I interferons (IFNs) constitute a group of proteins crucial for immune system function, particularly in response to viral infections.25,26,27 In patients with systemic lupus erythematosus (SLE), earlier studies have demonstrated significant activation of the type I interferon system, an observation considered unrelated to antiviral activity but closely associated with SLE disease activity.10 With the approval of Anifrolumab—a novel therapeutic monoclonal antibody developed to target and inhibit the type I interferon receptor, consequently mitigating the downstream effects of type I IFNs—in August 2021 in the United States, the role of type I interferons in SLE has recaptured the interest of both the scientific community and the general public.28
Patients with SLE exhibit increased expression of type I IFN-stimulated genes, collectively referred to as the “IFN signature”. This signature is associated with more severe disease manifestations and poorer outcomes.29 A component of this signature, IFI44L, displays significant demethylation in its promoter region among SLE patients, leading to upregulated expression.30 Dr. Lu’s team identified two CpG methylation sites within the IFI44L promoter region in blood samples that could serve as biomarkers for adult-onset SLE diagnosis.22 They subsequently developed a simple and efficient method for detecting IFI44L methylation, utilizing HRM-qPCR targeting these specific sites. This technique proved nearly identical to pyrosequencing, the gold standard for gene methylation assessment, and exhibited a sensitivity of 88.571% and a specificity of 97.087% for adult-onset SLE diagnosis in clinical samples.23 Nevertheless, additional research is required to ascertain whether IFI44L methylation analysis can be extended to cSLE diagnosis.
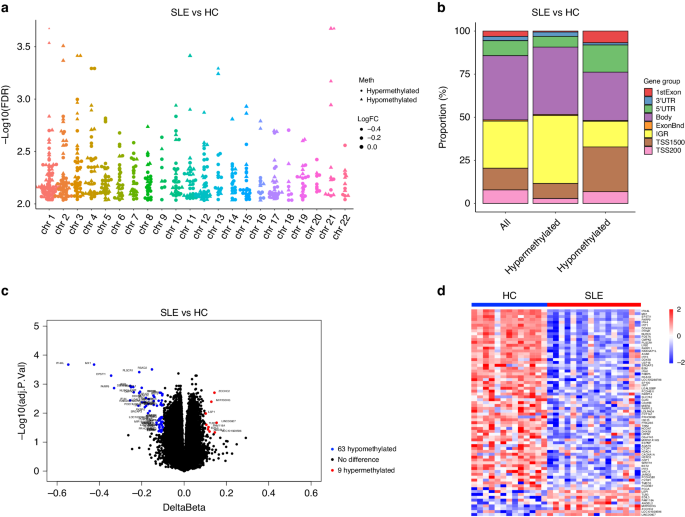
In this study, to investigate the diagnostic potential of IFI44L methylation in cSLE. We acquired whole blood DNA methylation and mRNA expression data from two cSLE study cohorts in the GEO database. By conducting differential analyses of DNA methylation and mRNA expression between healthy children and those with SLE, we identified DMGs and DEGs in cSLE patients. Upon overlapping hypomethylated DMGs and upregulated DEGs, we pinpointed 26 hypomethylated, highly expressed genes in cSLE. GO enrichment analysis of these 26 genes demonstrated a strong association with type I IFN, consistent with findings in adult-onset SLE. Among these overlapped genes, IFI44L exhibited the most pronounced differential expression and methylation, with a ∆β of −0.547 and a log2 fold change (FC) of 4.03, highlighting its potential as a biomarker for cSLE diagnosis. ROC curve analyses confirmed that the all 5 DMPs of IFI44L offered exceptional diagnostic accuracy for cSLE.
To evaluate the clinical utility of IFI44L methylation, we collected whole blood samples from 49 children with SLE and 12 healthy children, implementing the HRM-qPCR-based IFI44L methylation detection method reported in Dr. Lu’s study.23 Among the cSLE patients, 36 out of 49 exhibited low methylation levels in the IFI44L promoter region, while all 12 healthy children displayed high methylation levels. ROC curve analysis revealed an AUC of 0.867, a sensitivity of 0.753, and a specificity of 1.000, indicating that IFI44L DNA methylation could serve as an efficient blood biomarker for cSLE diagnosis.
In comparison to previous adult study utilizing HRM-qPCR for IFI44L methylation detection, our clinical study demonstrated a specificity of 1.000, which is comparable to adult-onset SLE. However, its sensitivity was only 0.753, notably lower than the adult value of 0.886.23 We offered two potential explanations to address this concern. First, the adult IFI44L methylation sites (Chr1: 79085222 and Chr1: 79085250) may not necessarily represent the optimal sites for cSLE. Our findings suggested that Chr1:79085586, Chr1:79085162, and Chr1:79085713, situated within 1500 bp upstream of the IFI44L transcription start site, might serve as more appropriate choices for cSLE. Consequently, while HRM-qPCR remains viable for detecting IFI44L methylation in cSLE, it necessitates the design of distinct primers based on unique methylation sites compared to those used for adult-onset SLE. Second, by comparing the clinical data between HRM-qPCR negative and positive patients, we found significant differences in SLEDAI scores, C3 concentrations, and anti-dsDNA titrations. This suggests a potential relationship between HRM-qPCR results and SLE disease activity. In our clinical study, some of the clinical samples were obtained from children with inactive or mild active SLE (SLEDAI ≤ 9),24 which may lower the positive detection rate of HRM-qPCR. However, it is crucial to emphasize that the widely-used SLEDAI score for adult disease activity assessment may not be ideally suited for cSLE. For example, cSLE exhibits increased severity in cardiopulmonary and renal manifestations, whereas the SLEDAI scoring system inadequately evaluates cardiac and pulmonary lesions and offers only a generalized assessment of renal damage, failing to reflect kidney impairment severity at a pathological level. Hence, the ability of HRM-qPCR to accurately represent cSLE disease activity necessitates further exploration upon the development of a more precise and comprehensive cSLE activity evaluation system.
This study still had several limitations. First, we collected specimens from only 49 children with SLE, potentially introducing random errors into our results. Second, our study focused exclusively on comparing children with SLE to healthy children, overlooking a comprehensive and systematic investigation of various diseases that necessitate differentiation from cSLE in clinical pediatrics, including juvenile idiopathic arthritis, Kawasaki disease, dermatomyositis, polymyositis, Sjögren’s syndrome, systemic sclerosis, cytomegalovirus infection, and drug-induced lupus, etc. These limitations are scheduled to be addressed in our forthcoming clinical studies.


留言 (0)