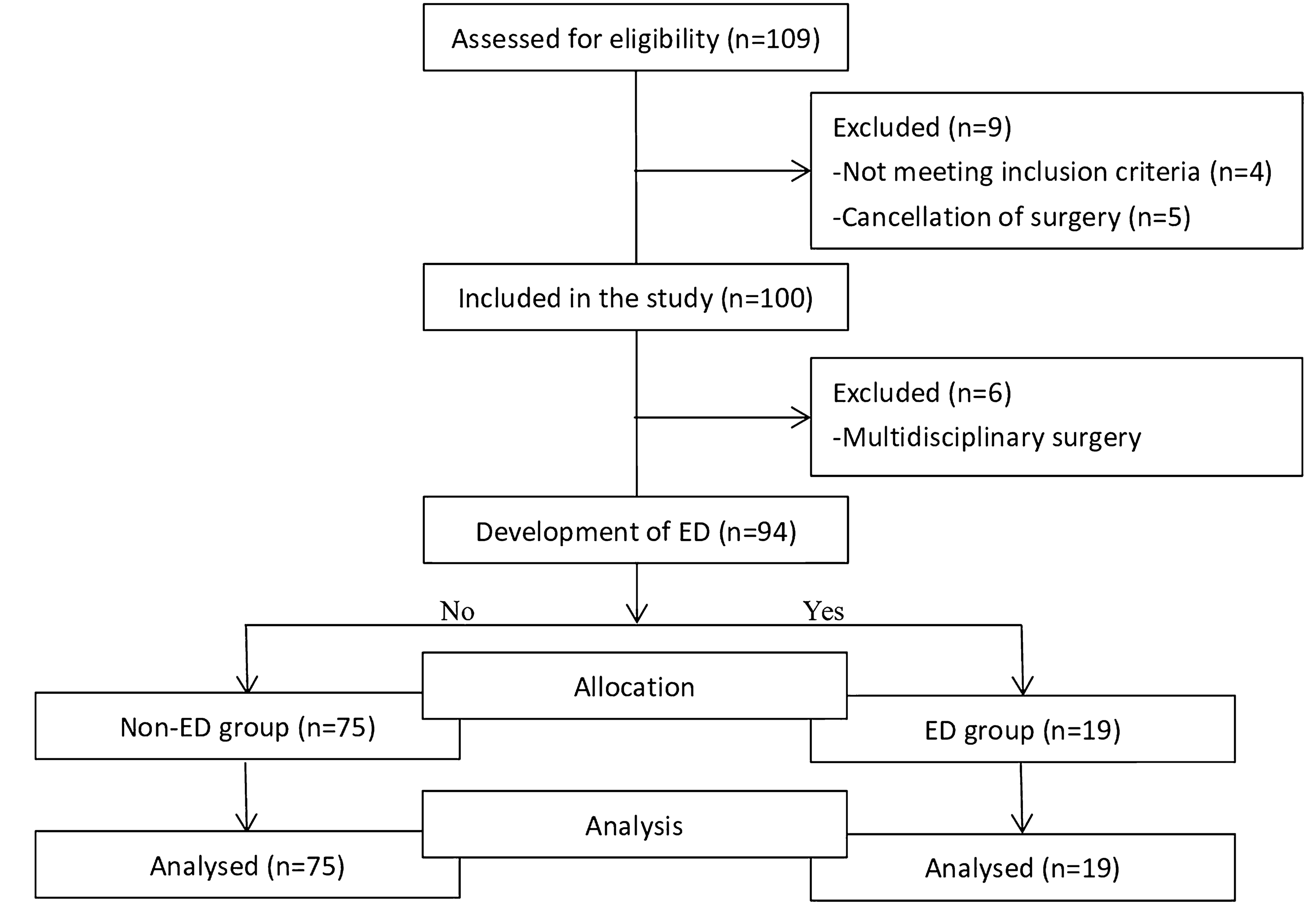
This report comprises a secondary publication based on additional data that were collected during a single-center randomized controlled trial undertaken between September 2018 and May 2019 at the Royal Brisbane and Women’s Hospital [4]. The trial was ethics-approved (HREC-18-QPCH-9 approved 21-03-2018), registered (ANZCTR 12618000445279) and participants provided written informed consent. Measurement of TcCO2 was stated in the trial registration and included in the initial ethical approval. We tested the hypothesis that the use of Optiflow THRIVE™ (Fisher & Paykel Healthcare, Auckland, New Zealand) at 70 L/min would increase the time to hypoxia and increase carbon dioxide elimination in apneic obese patients, when compared with 4 L/min oxygen administered via standard nasal prongs. The 42 participants were undergoing laparoscopic bariatric surgery, had BMI ranging from 38 to 68 kg/m2 and a mean (SD) PaCO2 at the end of apnea of 51.4 mmHg (7.5) (range 27.2–64.8 mmHg). The full inclusion and exclusion criteria and detailed methodology are available [4].
All participants were monitored according to local standards, with the addition of invasive radial arterial catheters. Participants were randomized to Group T, in which they were administered high flow nasal oxygen using Optiflow THRIVE™ at 70 L/min, humidified using the Fisher & Paykel 950 humidifier, providing 70% relative humidity (oxygen concentration delivered at 100%); or to Group N, in which they were administered standard nasal prongs at 4 L/min (Salter Labs, Arvin, CA, USA). In both groups, pre-oxygenation occurred in the ramped position and with FiO2 1.0 at 10 L/min.
Induction medications consisted of an opioid, propofol, and rocuronium with dosing at the discretion of the anesthetist. Anesthesia maintenance was achieved using propofol target controlled infusion. The patients were bag-mask ventilated to achieve an end-tidal oxygen fraction > 0.9. At this point, nasal oxygenation was applied according to group allocation and airway patency maintained using an oropharyngeal airway and two-handed airway maneuvers (chin lift, head tilt, jaw thrust).
Clinical observations and sampling occurred while the participants were anesthetized and apneic. TcCO2 was measured using the TCM5 FLEX transcutaneous monitor TC Sensor 92 and 32mm TOSCA fixation ring (Radiometer Pacific Pty. Ltd., Waverley, Victoria, Australia). The device sensor was calibrated for each patient, to reach the required temperature of 43.5 degrees Celsius. The participant’s skin was prepared with 70% isopropyl alcohol prior to placing the fixation ring over the clavicle and a small amount of contact gel applied before sensor attachment. Sensor membranes were replaced every three days. Arterial blood gas samples and TcCO2 measurements were obtained at baseline (prior to induction to anesthesia), at the start of apnea (T0), and the end of apnea (Tend). Tend was defined as the time at which peripheral arterial oxygen saturations (measured by pulse oximetry) dropped to ≤ 95% or a total of 360s of apnea, whichever occurred first. Participant characteristics were collected and these included age, sex, BMI, and co-morbidities including obstructive sleep apnea.
The sample size was a convenience sample of 42, determined according to the primary outcome of the original study [4]. The original analyses demonstrated no statistical differences between Group T and Group N in terms of the median PaCO2 post apnea or the rate of increase of PaCO2 during apnea. Therefore, for this methods comparison analysis, 42 participants were analyzed as one group. Agreement between PaCO2 and TcCO2 at the three time points was assessed using a non-parametric difference plot. Bias was reported as the median of the mean differences for each participant, with 95% confidence intervals (CI). The 95% limits of agreement (LOA) were estimated by the 2.5th and 97.5th percentiles with 90% CI, using quantile regression with cluster-robust bootstrap inference [5,6,7]. Analyses were run in R statistical package version 4.1.3.

留言 (0)