
Remember me
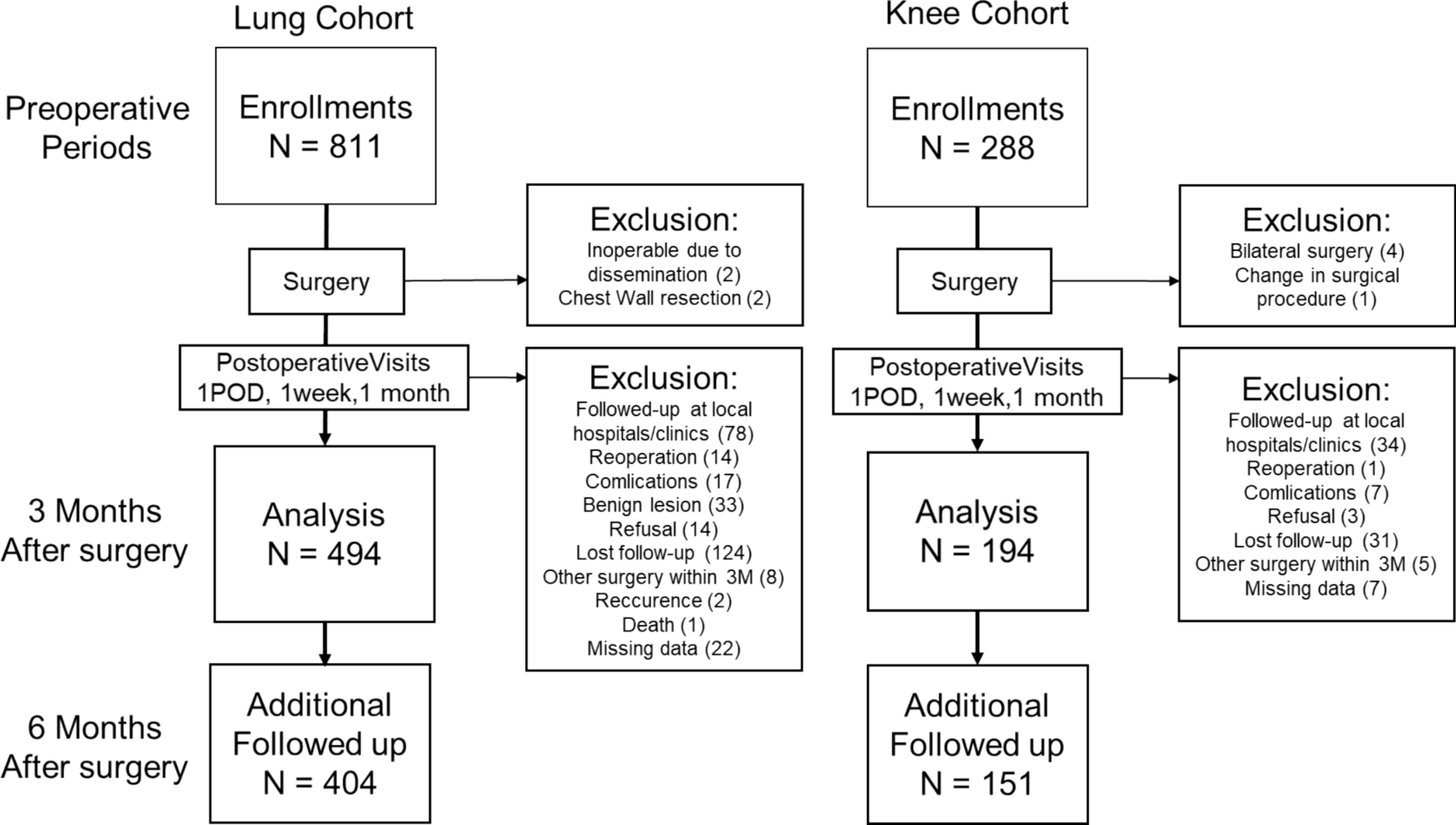

This survey was conducted by a web research company (Rakuten Insight, Tokyo). The survey was administered to 2000 consenting panel monitors (aged, 20–69 years) in the general population who had experienced pain anywhere in the body from October to November 2020. This online system for this study only collected data from respondents who completed the questionnaire. The questionnaire took approximately 20–30 min to complete. We excluded 169 participants who were receiving treatment for comorbidities (31 with cancer, 19 with stroke, 86 with depression, 13 with schizophrenia, 50 with psychiatric disorders other than depression and schizophrenia, and 30 with multiple diseases listed above). Furthermore, because e-cigarettes in Japan do not contain nicotine (though heated tobacco products do) and this study seeks to test a hypothesis about the effects of nicotine in cigarettes on the central nervous system, the nine e-cigarette users were excluded for a total of 1822 participants (Fig. 1). Based on a previous epidemiological study that examined the relationship between smoking and pain among 1189 Japanese workers [3], we established a sample size of approximately double for this study.
Fig. 1
Participant enrollment process. Participants were recruited in 2020
Main survey itemsBasic characteristicsAge, sex, marital status, and equivalized income were examined. Marital status was divided into married (including remarriage), common-law marriage, unmarried, separated or divorced (no remarriage), and bereaved. Equivalized income was calculated by dividing annual household income by the square root of the number of family members. Poverty was defined with reference to the 2018 poverty line [12] as an equivalized income of less than 1.27 million yen.
Lifestyle and medical informationThe survey collected information on obesity, exercise habits, and comorbidities. Body mass index (BMI) was calculated by body weight in kg/(height in m)2; those over 25 were defined as overweight. We investigated whether respondents had regular exercise habits (exercise up to a light sweat for 30 min or more at a time, for 2 days or more a week, and for 1 year or more; yes or no).
Concerning comorbidities, we surveyed whether respondents were receiving treatment for hypertension, hyperlipidemia, or diabetes.
Duration of painDuration of pain was classified into: less than 1 month; 1 to 3 months; 3 to 6 months; 6 months to 1 year; and 1 year or longer. Chronic pain was defined using the ICD-11 as pain that persists for more than 3 months [13].
Catastrophic thinkingCatastrophic thinking is defined as an exaggerated negative “mental set” brought to bear during painful experiences [14], and this abnormal perception of pain may be involved in cases of intractable pain. The Pain Catastrophizing Scale (PCS) is a self-report questionnaire that assesses catastrophic thinking related to pain. It consists of 13 items, with each item rated on a five-point Likert-type scale (0 = never; 4 = always). The possible score range is from 0 to 52, with higher scores indicating more intense catastrophic thinking. The PCS comprises three subscales: 'ruminating', 'helplessness', and 'magnification' [15]. There have been reports of a correlation between smoking and the PCS [16]. Since there was a possibility that the PCS would be a confounding factor for this study, we examined the participants' PCS scores and adjusted for it in the statistical analysis. In this survey, we used the Japanese version of the PCS, which has been validated for reliability and validity previously [17].
Smoking statusThe survey divided smoking status into the following four categories: daily, occasionally, stopped smoking, and never smoked. It also asked respondents the age at which they began smoking and the number of cigarettes smoked per day. The Brinkman index is calculated by multiplying the number of cigarettes smoked per day by the number of years of smoking. If the number of years spent smoking was less than 1, the Brinkman index was calculated using 0.5 as the number of years of smoking.
Central sensitization symptomsCentral Sensitization Symptoms were assessed using Part A of the CSI, a self-administered questionnaire. Part A of the CSI comprehensively evaluates subjective symptoms common to Central Sensitization Symptoms, such as pain, fatigue, sleep disorders, anxiety, depression, and cognitive impairment [10]. CSI-A consists of 25 items, and the frequency of subjective symptoms is evaluated on a five-point Likert-type scale of 0 to 4 (0 = never; 4 = always), with a total score of 0 to 100 points and a cut-off value of 40 [10, 18]. The distribution of CSI scores is shown in Supplementary Fig. 1.
Time discount rate coefficientContinuous intake of nicotine induces desensitization of nicotine receptors, resulting in decreased function of the reward dopamine system, in which the reward system cannot be activated unless more nicotine is ingested [19]. However, it has also been reported that patients with chronic pain have reduced activity signals in the reward system regions of the brain, including the nucleus accumbens [20]. The time discount rate is involved in decision-making associated with the reward prediction function of the reward system (the process of deciding whether to prioritize immediate rewards or future rewards that are valuable to oneself) [21]. Since there was a possibility that the reward system would be a confounding factor for this study, the survey investigated the participants’ time discount rate coefficient. In response to the question, "For a gratuity of XXX yen paid today, would you feel that a gratuity of ¥YYY would be of equal value if it were paid ZZZ days later?", the survey instructed respondents to enter a numerical value into the "ZZZ" portion of the question. The survey included 10 items of this type, using somewhat different amounts each time. The functional form of the time discount coefficient uses a hyperbolic model of V(D) = V(0)/(1 + κD) [V(D): delayed reward (XXX), V(0): immediate reward (YYY), D: number of days (ZZZ), κ: time discount coefficient], and when plotting the hyperbola for each individual, the coefficient κ was calculated.
Statistical analysisThe explanatory variables were divided into two groups: a smoking group and a non-smoker group. Multiple regression analysis was performed using the CSI value as a continuous variable, ranging from 0 to 100 points, as the objective variable. Furthermore, these analyses were performed again after changing the smoking status to the Brinkman index.
A modified Poisson regression model was used to compare the relative risk (RR) and 95% confidence intervals (CIs) of exceeding the CSI cut-off score among smokers relative to nonsmokers. We used Statistical Analysis Software (SAS; SAS Institute Inc., Cary, NC, USA) version 9.4 and the REPEATED statement of SAS PROC GENMOD to estimate the sandwich error using the modified Poisson regression model.
In these analyses, Model 1 was adjusted for age and sex. Model 2 was further adjusted for BMI (quintile), marital status, equivalized income (quintile), regular exercise (yes/no), history of hypertension, history of hyperlipidemia, history of diabetes mellitus, and pain chronicity (defined as pain duration of 3 months or more). Model 3 included additional adjustments for the PCS score.
We excluded 120 participants with history of mental illnesses (such as depression, schizophrenia, and other psychiatric disorders) in our analysis to distinguish between major mental illnesses and central sensitivity syndromes (CSS). However, acknowledging the potential overlap between mental illnesses and CSS, we aimed to prevent misclassification. In the sensitivity analysis, we included these 120 participants, who were previously excluded from the main analysis due to their history of mental illnesses, which was considered a confounding factor. We re-ran the multiple regression analysis incorporating this group (n = 1942). In the sensitivity analysis, adjustments were made in Model 3, and further adjustments for the history of depression, history of schizophrenia, and history of other mental diseases were incorporated in Model 4.
SAS 9.4 was used for all the above data analysis, and statistical significance was set at p < 0.05 for both models.
Ethical concernsWhen administering the Internet survey, participants were presented with an explanatory letter outlining the survey, stating that the data would not be used for any other purpose, that their personal information would be protected through anonymization, and that they would not be disadvantaged if they refused to cooperate in the survey. Participants agreed to participate in the research by clicking the consent button and proceeding to the questionnaire response screen. Participants were incentivized with points that could be used for Internet shopping or converted to cash. The points awarded for survey cooperation are uniformly determined by the internet survey company, in accordance with established rules. However, researchers are not informed of the specific monetary value of this point system. This study was approved by the Ethics Committee of Juntendo University School of Medicine (approval number: 2020173, approval date: October 15, 2020).
Comments (0)