
Remember me

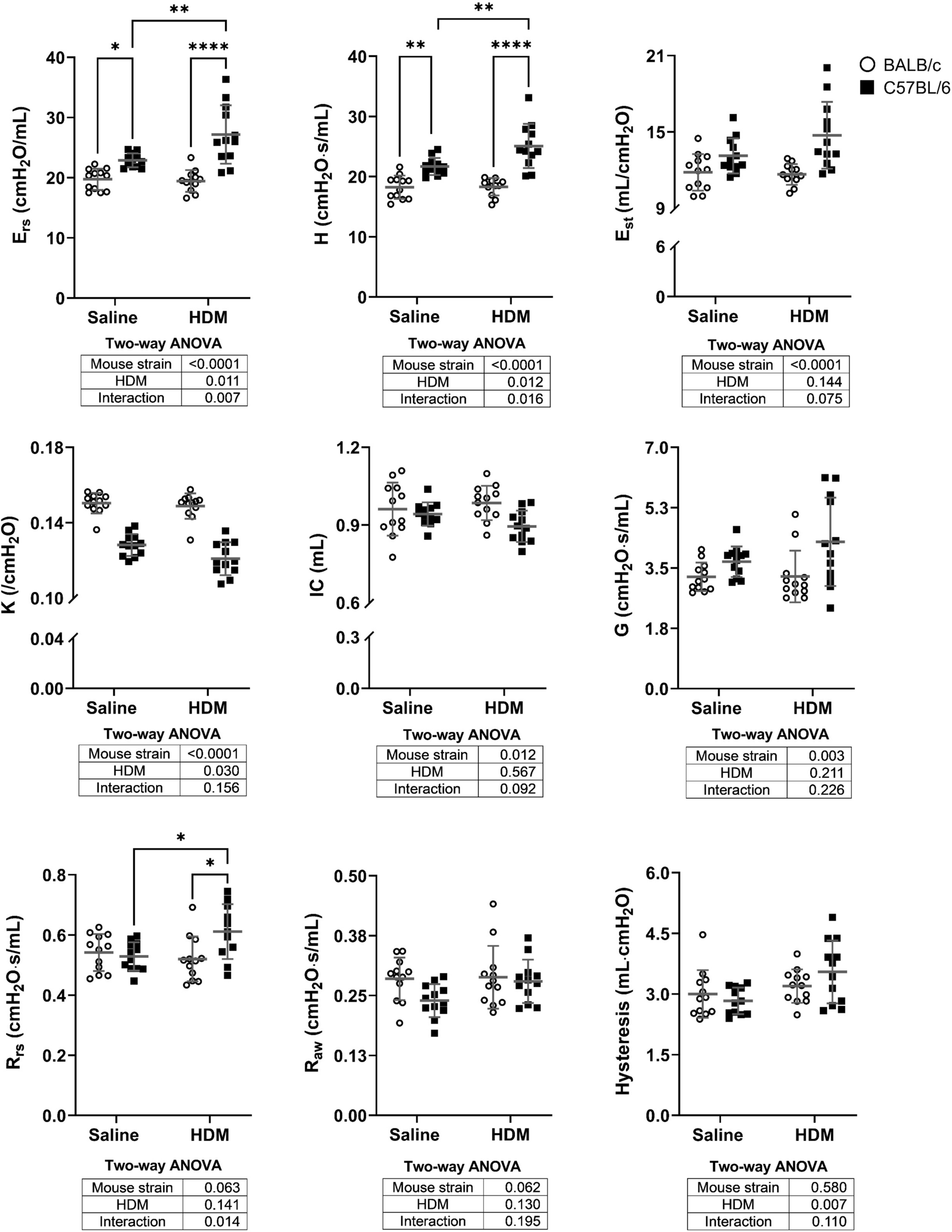




The results demonstrate that, among all baseline characteristics studied and depending on how the methacholine response was measured, lung tissue compliance and the inspiratory capacity were the most commonly and robustly associated with the methacholine response in BALB/c and C57BL/6 mice with and without experimental asthma. The results also demonstrate that all indicators of stiffness (Ers, H & Est) or its inverse, compliance (K), were markedly different between BALB/c and C57BL/6 mice (Fig. 1). This confirms our previous study in naïve mice, showing that lungs of C57BL/6 are stiffer than BALB/c mice not because of smaller lungs but truly due to a stiffer lung tissue associated with an increased collagen content [8]. Notably, the surface tension was not compared in that latter study, which will be required in future studies owing to its important impact on lung compliance [11]. The results presented herein still extend our previous findings [8] by showing that this striking interstrain difference in lung stiffness is conserved with experimental asthma.
The reason why IC was associated with the methacholine response is uncertain. It is possible that with bigger lungs, a greater amount of methacholine entered the lungs during the nebulized challenge [12]. The fact that IC was associated even when the response was monitored by measuring the changes in airway resistance (Raw), an indicator of airway narrowing, would support this conjecture. This is because the biggest fraction of nebulized methacholine entering the lungs is initially deposited in large airways [12]. Therefore, with a greater amount of methacholine getting into the lungs, this would imply that greater concentrations of methacholine are achieved in large airways, which would then further airway narrowing and amplify the changes in Raw. The link between IC in the methacholine response will obviously need to be further investigated.
The likely link between K, an indicator of lung tissue compliance [13, 14], and the response to nebulized methacholine seems more obvious. In our opinion, it is due to a reduced load impeding the shortening of the airway smooth muscle [15]. Indeed, with a more compliant lung tissue, it should be easier to stretch the lung parenchyma attached on the outer edge of the airway wall during bronchoconstriction, which should then lead to greater airway narrowing for any given smooth muscle force [15]. It is also likely that this extra narrowing would be potentiated in an asthmatic environment. This is because the constriction of the airway lumen is amplified by oedematous airway wall and the luminal accumulation of inflammatory, exudative, and mucosal fluids [16]. Finally, and most importantly, a stiffer tissue may force the lungs to work more homogeneously and thereby prevents hyperresponsiveness by protecting against airway narrowing heterogeneity and closure, which are the main causes of hyperresponsiveness in asthma and experimental asthma [17,18,19,20,21,22,23,24,25,26].
Importantly, among all variables that are highly linearly correlated, LASSO typically selects only one, effectively simplifying the model by eliminating some variables. K was highly, and expectedly, correlated with Ers, H, and Est. Indeed, K being a volume-independent indicator of lung tissue elastance [13, 14], the lung feature it represents is somewhat embedded in any indicator of lung stiffness (Ers, H, and Est). The fact that LASSO selected K instead of these other colinear characteristics is interpreted herein as a sign that K better defines the feature of the lungs that is best associated with the methacholine response. Yet, it is acknowledged that K can be substituted by Ers, H, or Est in our analyses without losing much of the models predictability. This essentially means that although K was selected in our analyses, lung stiffness in general was strongly associated with the methacholine response, irrespective on how it was measured or the specific parameter that was used for appraising it (K, Ers, H, or Est).
Another important limitation in our multivariate analyses is that the significant effect of stiffness was driven by mouse strains. This group effect is consistent with our two previous studies [6, 8], showing high lung elastance and low methacholine responsiveness in C57BL/6 mice and, inversely, low lung elastance and high methacholine responsiveness in BALB/c mice. However, it also implies that what we are reporting herein are mere associations. Any other features than lung stiffness that are strikingly different between these two mouse strains may potentially explained, partially or totally, their markedly different levels of response to methacholine.
We thus proposed that the greater lung tissue compliance of BALB/c mice predisposes to excessive airway narrowing because it reduces the load impeding smooth muscle shortening, which may then yield a catastrophic response to methacholine when combined with other ‘asthmatic’ lung alterations (Fig. 2). Inversely, the stiffer lung tissue of C57BL/6 mice should protect against airway narrowing by increasing the load impeding smooth muscle shortening, thereby mitigating the methacholine response, especially in the context of experimental asthma.
Fig. 2
The catastrophic response to nebulized methacholine in BALB/c mice with experimental asthma stems from a more compliant lung tissue, conspiring with inflammatory obstruction during smooth muscle shortening to promote excessive luminal airway narrowing. Spring thickness represents parenchymal lung stiffness. Mucus/inflammation, lamina propria and muscle are yellow, grey, and black, respectively
It is worth mentioning that human asthma is not typically associated with altered lung tissue compliance. Exceptions exist though. More persistent and severe asthma, often in the elderly, is sometimes associated with increased lung compliance [27,28,29,30,31,32]. Perhaps the BALB/c would be a good choice of mouse strains for studying hyperresponsiveness in this subgroup of asthmatics, or in subgroups presenting emphysema, such as in patients with an asthma-COPD overlap syndrome. Nonetheless, an important cause of hyperresponsiveness in BALB/c mice with experimental asthma may be irrelevant to hyperresponsiveness in most asthmatic individuals. This also suggests that even if a specific trait, such as hyperresponsiveness, resembles human asthma in a mouse strain, the underlying causes are not necessarily the same.
Comments (0)