
Remember me





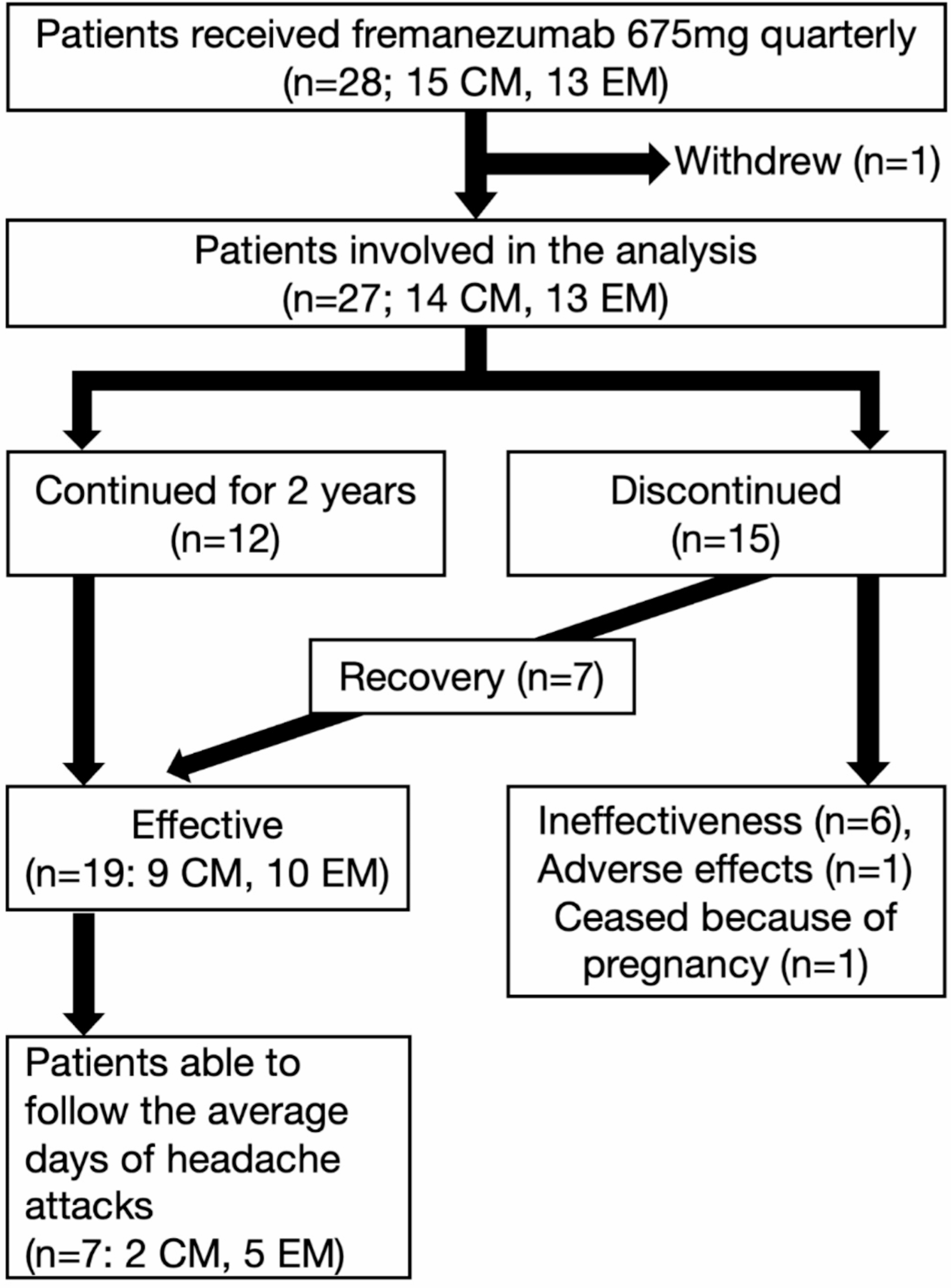

A total of 130 patients received at least one intravenous infusion of eptinezumab during the audit period (Fig. 1). Of these, eight patients had other headache or facial pain conditions refractory to medical management but displayed some associated symptoms often described in migraine, namely photo-phonophobia, motion sensitivity and/or had a migraine biology (personal and/or family history of migraine). Completed headache diaries and HIT-6 at baseline were obtained from 121 patients [102 female; mean age, 44.7 Standard Deviation (SD) ± 13.5 years]. At the time of analysis for this report, 119 patients had their diary submitted to the clinic as part of their three-month follow up. Eighty-two patients received at least two eptinezumab treatments of which 76 had a six-month follow-up.
Demographic and clinical characteristics of the patients’ group included in the analysis at baseline are summarised in Table 1. All patients were medically refractory or resistant according to the European Headache Federation (EHF) consensus [15]. Eighty patients (67%) displayed a suboptimal response to one or more different anti-CGRP pathway mAb. Half of the patients reported a daily headache pattern at baseline. Of the 119 patients, 32 (27%) were classified as patients with medication overuse. At the time of the first infusion 72 (60%) of patients were taking concomitant preventive treatments; three-patients were on three-monthly onabotulinum toxin A injections when they initiated eptinezumab. Eighty-seven patients (73%) reported at least one comorbidity.
Table 1 Demographic and clinical characteristics at baseline of 119 migraine patients treated with EptinezumabEfficacy outcomes after first eptinezumab infusion – 3 months follow-upOverall, during the entire 3-month observation period post-treatment initiation, MMD days and MHD were significantly reduced compared to baseline (MMDs: F3.6, 252.6 = 10.4, P < 0.00; MHDs: F2.6, 194.8 = 55.6, P < 0.001), as well as the number of abortive treatment intake days (F5.2, 343.2 = 2.5, P = 0.03). Additionally, the HIT-6 score was significantly reduced across the entire observational period (F6.0, 102 = 2.3, P = 0.04) (Fig. 2).
Fig. 2
Three-month outcomes on all patients treated with eptinezumab. P values are indicated in the graphs; *, P < 0.001
Compared to baseline, the mean reduction in MMD over the three-month period was 5.4 days (from 17.9 ± 0.8 to 12.5 ± 0.5; t109 = −4.4, P < 0.001). The mean reduction in MHD was 2.7 days (from 26.7 ± 0.5 to 24.2 ± 0.4; t109 = −2.2, P = 0.03). Treatment with eptinezumab also increased the number of headache-free days per month by 2.8 ± 0.5 days (P = 0.006). The mean number of abortive treatment days was reduced across the three-month period (from 11.9 ± 0.9 to 8.9 ± 0.5; t99 = −2.7, P = 0.009). Compared to baseline, the reduction of mean HIT-6 score was 5.3 points at month 3 (from 69.4 ± 0.6 to 64.0 ± 0.4; t93 = −5.3, P < 0.001).
At month 1, 2 and 3, 50% (N = 59), 53% (N = 63) and 53% (N = 63) of patients obtained at least a 30% reduction in MMD, respectively. The percentage of patients who achieved at least a 50% reduction in MMD at months 1, 2 and 3 were 36% (N = 43), 39% (N = 46) and 37% (N = 44), respectively (Fig. 3). Considering the average reduction in MMDs across the three months for the 119 patients, 61 (51%), 41 (35%) and 15 (13%) of patients achieved at least a 30%, 50% and 75% reduction in their mean migraine days, respectively. Thirty-six patients (30%) discontinued the treatment due to lack of efficacy (N = 30) or side effects (N = 6). One patient continued treatment at a local clinic and was discharge from our service.
Fig. 3
Six-month outcomes on all patients treated with eptinezumab. P values are indicated in the graphs; *, P < 0.001
Twenty-one patients who achieved less than 30% reduction in MMD across the 3-month period but had some benefit either in migraine associated symptoms or in their HIT-6 scores were offered a second infusion.
Efficacy outcomes after second eptinezumab infusion – 6 months follow-upA total of 82 patients received a second eptinezumab infusion. Of those, at the time of the analysis, 76 patients had their 6-month follow up review. Overall, during the entire 3-month observation period post-second eptinezumab infusion initiation, MMD, MHD and abortive intake days were significantly reduced compared to baseline. Additionally, the HIT-6 score was significantly reduced across the entire observational period (Fig. 3).
Compared to their baseline, the mean reduction in MMD over the three-month period following the second infusion of eptinezumab was 6.3 days (from 15.5 ± 1.0 at baseline to 9.2 ± 0.5; t81= −6.7, P < 0.001). The mean reduction in MHD was 5.3 days (from 26.0 ± 0.8 at baseline to 20.8 ± 0.6; t81= −3.1, P = 0.003). There was an increment of the number of headache-free days by 5.3 days (P < 0.001). The mean reduction in abortive treatment days was significant across the three-month period (from 12.8 ± 1.2 at baseline to 8.0 ± 0.6; t81= −3.7, P < 0.001). Compared to baseline, the reduction of mean HIT-6 score at month 6 was 6.3 points from 68.9 ± 1.3 to 62.6 ± 0.7; t73= −5.0, P < 0.001).
At month 4, 5 and 6, 66% (N = 50), 65% (N = 49) and 62% (N = 47) of patients obtained at least a 30% reduction in MMD, respectively. The percentage of patients who achieved at least a 50% reduction in MMD at months 4, 5 and 6 were 51% (N = 39), 50% (N = 38) and 41% (N = 31), respectively (Fig. 3). Considering the average reduction in MMD across the three months for the 76 patients, 48 (63%), 33 (43%) and 14 (18%) of patients achieved at least a 30%, 50% and 75% reduction, respectively, in their mean monthly migraine days.
Of the 21 patients who achieved less than 30% reduction in mean MMD across the 3-month period, and continued to have a second eptinezumab infusion, ten patients (48%) achieved at least a 30% reduction in mean MMD across the 3-month following the second eptinezumab treatment.
After the second infusion, 15 (20%) patients discontinued the treatment due to inefficacy, as there was no reduction in MMD across the three months (from 17.8 ± 0.5 at baseline to 16.7 ± 0.5 MMD across three months). Of these, 11 belong to the group who did not respond to the first infusion and continued to have the second one, hence four patients (5%) who responded to the first infusion, did not benefit from the second infusion.
The percentage of 30%, 50% and 75% responders across the six months of treatments, and the overall responder rates per 3-monthly periods and across all patients is shown in Fig. 4.
Fig. 4
Percentage of 30%−50%−75% responders across the six months of treatments, and the overall responder rates across all patients
Effectiveness of IV eptinezumab in patients previously treated with one or more anti-CGRP pathway mAbsThirthy-two out of 80 patients who did not respond to at least one anti-CGRP pathway mAb (40%; 1 CGRP mAb failure: N = 21/80, 2 CGRP mAb failures: N = 11/80) achieved at least a 30% reduction in their mean MMD after the first eptinezumab infusion, and 26 (33%; 1 CGRP mAb failure: N = 18/80, 2 CGRP mAb failures: N = 8/80) of them continued to respond to eptinezumab after the second infusion. Of the CGRP mAbs naïve patients (N = 39/119), 29 patients (74%, all CM patients) achieved at least a 30% reduction in their mean MMD after the first eptinezumab infusion, and 22 patients (56%) continued to respond to eptinezumab after the second infusion. A chi-square test of independence was performed to examine the relation between CGRP naïve/prior CGRP failure and the 30% responder rate. The relation between these variables was significant, X2 (1, N = 119) = 12.30, p = 0.0001. CGRP-naïve patients were more likely to achieve at least a 30% reduction of MMD than those who failed to respond to previous CGRP mAbs.
Effectiveness of IV eptinezumab in patients with chronic daily headacheOf the patients (50%) who reported a chronic daily headache pattern at baseline (Baseline MD: 19.9 ± 1.1; baseline HD: 30.0 ± 0.03), 24 (41%) and 18 (31%) achieved at least a 30% and 50% reduction in their mean MMD, correspondingly, after the first infusion of eptinezumab. Of the patients who did not have a daily headache pattern at baseline (baseline MD: 17.0 ± 1.0; baseline HD: 24.5 ± 0.5), 37 (62%) and 23 (38%) achieved at least a 30% and 50% reduction in their mean MMD, correspondingly, after the first infusion of eptinezumab. At six months, 22 (37%) and 17 (28%) of the CDH patients continue to have at least a 30% and 50% reduction in their mean MMD. Of the patients who did not have a daily headache pattern at baseline, 26 (43%) and 16 (26%) achieved at least a 30% and 50% reduction in their mean MMD, correspondingly, after the second infusion of eptinezumab. No association was found between the baseline headache pattern (daily/non-daily) and responders rate following the first or second eptinezumab infusion (p ≥ 0.18).
Safety and tolerabilityAfter one infusion of Eptinezumab, 24 patients (20%) reported at least one adverse event. A total of 34 adverse events were reported by the patients after the first infusion. Nine patient reported at least one adverse events after the second infusion (Table 2). Adverse events were transient, lasting up to two weeks post-injection and described as mild or moderate. However, six patients (5%) discontinued the treatment because of side effects (cold/flu symptoms, raised blood pressure, which was found subsequently to be due to previously undiagnosed hypertension, atypical chest pain, headache worsening). The raised blood pressure was the only adverse event that occurred immediately after the eptinezumab infusion.
Table 2 Percentage of adverse events after first and second eptinezumab infusions
Comments (0)